 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
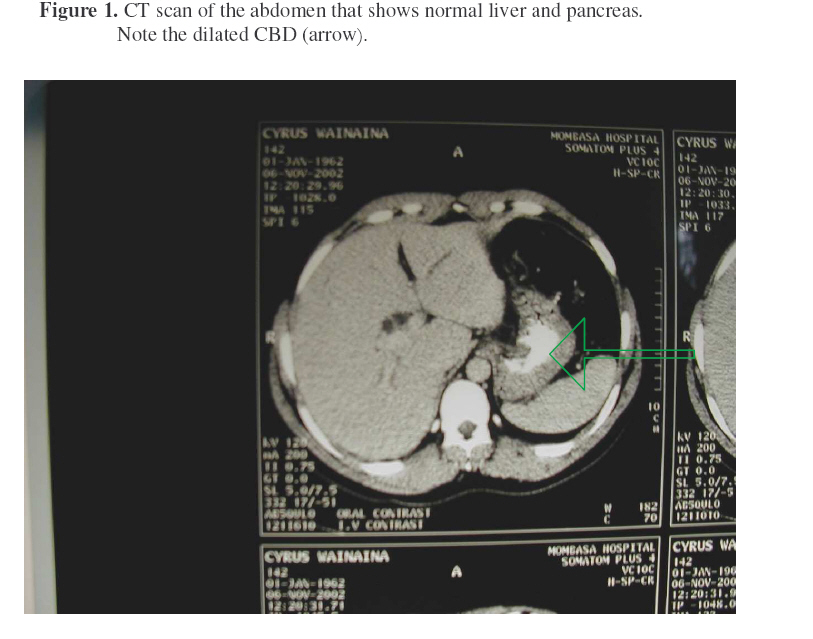
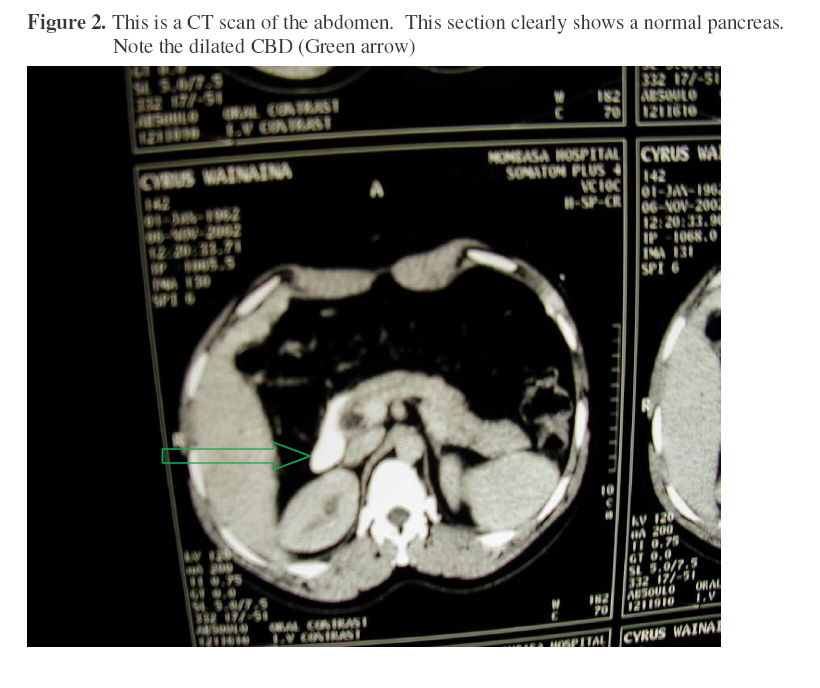
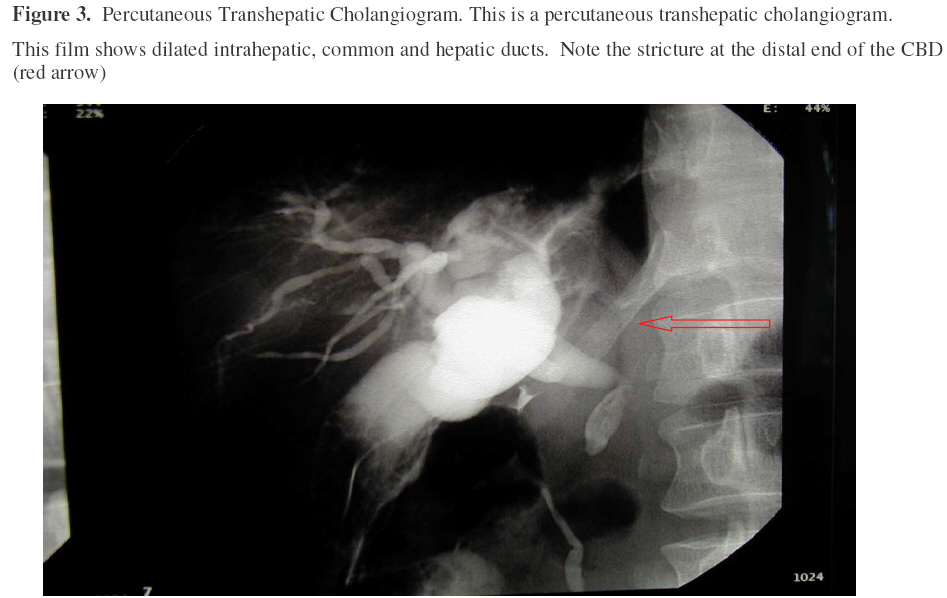
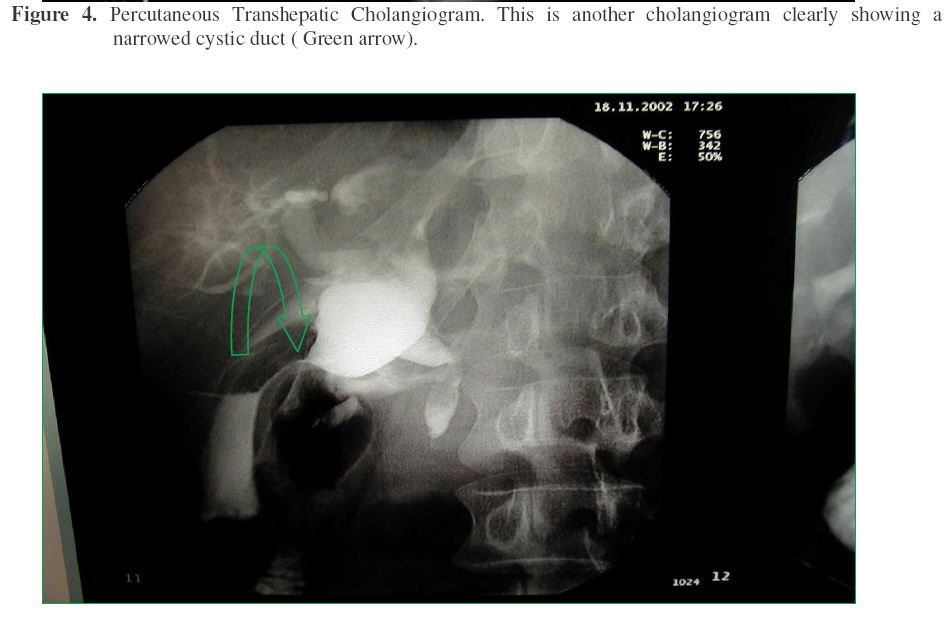
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 154-158 Mirizzi Syndrome: A Case Report Muthuuri, J. M.: MB.ChB, MMed (Surg), FCS (ECSA). Consultant General & Trauma Surgeon Correspondence To: Dr J. M. Muthuuri, The Mombasa Hospital Private Clinics P.O. Box 84074 Code Number: js07028 IntroductionThe classical Mirizzi Syndrome described by P. L. Mirizzi in 1948 is characterized by a cholecystocholedochal fistula arising from a calculus in the cystic duct that erodes into the common hepatic duct. The gall bladder eventually collapses due to fibrosis while the terminal bile ducts become dilated. A calculus is usually found in the cystic duct or in the Hartman’s pouch. This presents an unusual and specific cause of obstruction of the terminal bile ducts. Patients present with obstructive jaundice. Cholangiography shows narrowing of the common bile duct at the porta hepatis, which can have the appearance of a cholangiocarcinoma. Preoperative ERCP is helpful in deciding the best type of operative approach. The true pathology is eventually identified at surgery. The operation is often difficult because of severe inflammation and fibrosis. For cholecystocholedochal fistula, a cholecystoduodenostomy is a safer operation. In more complex situations a choledochoplasty (using part of the gallbladder wall) or a choledochojejunostomy Rouxen-Y may be required. Case Report CW, a 39-year-old male, non-diabetic was referred to us with a one-month history of jaundice, generalized body itching and loss of weight. There was a history of heartburn but no nausea or vomiting. He would get constipation followed by episodes of diarrhea. He had of late lost appetite. His stools were pale and urine was deep yellow.Past medical history was non-significant. There was no history of jaundice prior to this illness. He did not smoke but drank alcohol occasionally. He worked as a technician in a photocopying business. On examination, he was in good general condition. He was 170 cm tall and weighed 65kg. He had a generalized papular rash from scratching. He had deep jaundice but no pallor or lymphadenopathy. The abdomen was soft with no ascites. The liver and spleen were not enlarged. The gallbladder was palpable and mildly tender with a positive Murphy’s sign. The rest of the examination was normal. A clinical diagnosis of obstructive jaundice possibly due to a periampullary tumour was made. The results of investigations were: Haemoglobin of 14.3g/dl, WBC 4,200mm3 , ESR 48mm/hr, platelets 399,000. There were no malaria parasites. Random blood sugar on first admission was 6.3mmol/l. Urinalysis showed some bilirubin but no urobilinogen, proteins, sugar, blood or pus cells. Liver function tests showed a total bilirubin of 221umol/L with direct bilirubin of 141umol/L. Alkaline phosphatase was raised 935lU/L. The enzymes (SGOT, SGPT, and Gamma GT) were moderately elevated. Hepatitis BsAg, Hepatitis C and HIV tests were negative. The prothrombin time, serum urea, creatinine and electrolytes were within normal range. Abdominal ultrasound showed a normal gallbladder, the intrahepatic biliary ducts were normal but the common bile duct (CBD) was dilated. CT scan confirmed a dilated CBD (Figure 1). The pancreatic head was prominent (Figure 2). There were vague masses in the para aortic region, possibly lymph nodes. Scrotal ultrasound scan showed normal testis. ERCP and Percutaneous Cholangiography were not done At operation, the gallbladder was found distended, with no calculi. No calculi were palpable in the CBD. The head of pancreas felt nodular but not enlarged. A biopsy was taken. The ampulla of Vater was open and draining clear fluid. There were no calculi. A billiary diversion was done with a cholecystojejunostomy. Post-operative recovery was uneventful. The jaundice cleared completely within about 20 days. Histology from the pancreatic biopsy showed normal pancreatic tissue with no evidence of malignancy. A follow up CT scans of the abdomen done three months later was normal. Follow Up Nine months after the operation, he came back to see me with recurrent jaundice, fever and itch. There were no abdominal masses or organomegaly. Liver function tests showed marked elevation of total and direct bilirubin and all the liver enzymes especially alkaline phosphatase and gamma and gamma GT. Repeat spiral CT scans (Figures 1 and 2) were reported to show dilated CBD. The pancreatic head was normal. He was referred to a gastroenterologist for opinion, ERCP and Cholangiography. ERCP was not done. A percutaneous Transhepatic Cholangiography (PTC) (Figures 3 and 4) were reported to show “Choledochojejunostomy, which showed good drainage into the jejunum. There were multiple filling defects in the gallbladder, which were consistent with air bubbles. The common hepatic duct and CBD were dilated. There was a smooth stricture at the distal end of the CBD, consistent with benign stricture”. He was prescribed a course of antibiotics after which he appeared to improve and jaundice partly cleared. However, jaundice and itch quickly returned. He was also loosing weight fast. He returned for review four months later. Meanwhile he had rapaciously chewed sugarcane and drunk a lot of sugarcane juice in an attempt to “cure” as he had been advised by well-wishers. A review of the cholangiograms gave away the diagnosis. He consented for operation. Preoperative investigations revealed high blood sugar (25.4mmol/l). The pancreatic enzymes were within normal limits. The LFTS had not changed much from previous figures shown above. The prothrombin time was within the normal range. The blood sugar was easily controlled with insulin. At re-exploration, the liver, spleen and pancreas were found to be normal. The gall bladder was thickened and contracted. The common hepatic duct and the common bile ducts were grossly distended, forming a large sac. The cystic duct was thin and tough. Attempts to cannulate it failed. The ballooned sac was opened to review distended CHD, CBD and both the right and left hepatic ducts. There was a lot of sludge, which was cleaned off. The CBD was completely blocked distally (the retroduodenal portion). Choledochojejunostomy was performed. The remnant of the collapsed gall bladder was removed. Post operatively he recovered without any problem. The jaundice cleared in a few days He was back to work in four weeks. I have followed him up for eight months now. He is fine. Discussion Lithiasis in general is uncommon in indigenous African men. We see more gall bladder stone disease in immigrant population of Asian and Arabic descent. In populations where lithiasis is common, calculi in the bile duct may lie dormant for many years and only come to light because of an episode of pain, jaundice, or cholangitis. They may also be discovered by abdominal ultrasonography during routine scanning. Between 8 and 15 per cent of patients with stones in the gallbladder also have stones in the ducts1. Females are more affected than males. The incidence increases with age. Mirizzi syndrome is more common in the elderly, but any patient with cholelithiasis is at risk2 . Our patient was 38 years old man at presentation. Three cases aged 49, 58 and 59 years have been reported by Toufeeq3 . Primary stones form within the bile duct. They are usually bilirubinate stones of the soft brown type, and they are associated with biliary stasis due to obstruction, infection and the presence of foreign bodies such as food. In the Orient they may be caused by infection, sometimes associated with parasites within the biliary tract. However, most common duct stones originate in the gallbladder and migrate through the cystic duct into the common bile duct. These secondary stones consist mostly of cholesterol and often grow in size within the duct. We have not established the cause of lithiasis in him. Mirizzi Syndrome has no consistent or unique clinical features that distinguish it from other more common forms of obstructive jaundice. Symptoms of recurrent cholangitis, jaundice, right upper quadrant pain and abnormal liver function tests may or may not be present4. Patient may present acutely with pancreatitis or cholecystitis. Our patient presented with jaundice. He had no pain or fever initially. These symptoms set in later with increasing derangement of the liver function tests. We suspect he became diabetic because of taking too much sugar (sugar cane). The most important investigation is ultrasound examination of the liver, the bile duct, the gallbladder and the pancreas. The ultrasonographer need only decide whether or not the bile ducts are dilated. The normal common bile duct should not be greater than 7mm in diameter when measured on ultrasound. Signs of dilatation of the biliary duct system including the CHD, CBD and abrupt narrowing of the CBD are good indicators. Impacted stone may or may not be visualized. There was biliary dilatation especially of the CHD and CBD in our patient. Intrahepatic ducts were reported normal. CT scan has a limited place in the imaging of common duct stones. The ultrasound examination may raise the possibility of a malignant obstruction, and a CT will very reliably detect dilation of the ducts and identify the site and the cause of an obstruction. In this case CT scan actually showed dilated CBD (Figures 1 & 2). No calculus was seen. The pancreatic head was initially reported to be prominent with vague masses in the para aortic region (nodes?). This error led to a wrong operation being performed. Cholangiography demonstrates the narrowing of the distal CHD and of the proximal CBD as well as, in some instances, the dilatation of the proximal biliary duct system. Cholangiography gives excellent anatomical visualization. Cholangiography was done late in this case. Percutaneous transhepatic cholangiography (PTC) was reported to show dilated CHD and CBD. There was a smooth stricture at the distal end of the CBD, which was consistent with benign stricture (Figures 3 & 4). At this point the diagnosis was suspected. Liver function tests are usually abnormal. Apart from elevated bilirubin levels, the only other distinguishing abnormality is the high levels of alkaline phosphatase and gamma GT. However, serology for viral hepatitis must be done to rule out concurrent infection. It is also prudent to do pancreatic enzymes. In this case, liver function tests were consistently and progressively abnormal. An attempt has been made at classification of the Mirizzi syndrome3,5 . This classification is more of a division of the same condition in it’s various stages, so that type I describes the condition before fistula formation, while type II – IV, a fistula is present but is of different size in relation to the size of the CBD5. I did not attempt to classify this case. Most authors agree that the treatment of choice for Mirizzi syndrome is surgical1,4,6,7 . However, electrohydraulic lithotripsy (EHL) was reportedly successful in 38 of 38 patients with known Mirizzi syndrome8. The technique used in surgical treatment will depend on the stage of the patient’s condition, hence, the attempt to classify Mirizzi syndrome. The stage may however, not be obvious until the procedure has begun. That is why pre-operative Cholangiography is indicated to visualize the anatomy and the stage of the disease i.e. presence or absence of fistula. When there is compression without a fistula it is generally treated with cholecystectomy and choledochoduodenostomy. When there is a fistula formation a biliary enteric bypass via Roux-en-Y choledochojejunostomy is the most suitable. Note however, that intrahepatic lithiasis has been reported after cholecystojejunostomy9. This patient initially had Cholecystojejunostomy done for biliary bypass. By then the cystic duct was patent and draining, but later blocked as fibrosis progressed. This has been shown to be the progressive outcome in most of these cases5. Definitive procedure of Roux-en-Y choledochojejunostomy was carried out after the diagnosis became clear. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07028f4.jpg] [js07028f3.jpg] [js07028f2.jpg] [js07028f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}