 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
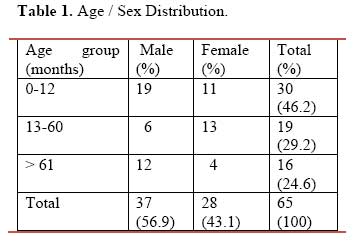
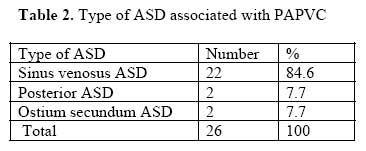
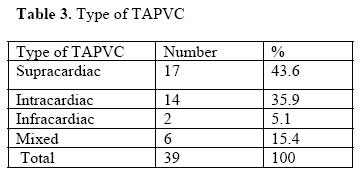
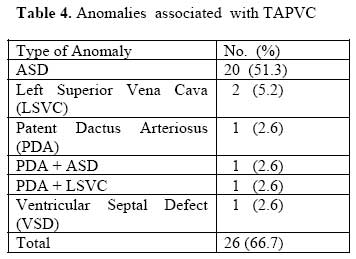
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 18-22 Patterns of Anomalous pulmonary Venous Connection as Seen at Care Hospital, Hyderabad - India. E.V. Ussiri1,2, E.T.M. Nyawawa1, G.C. Mannam2, L.R. Sajja2 , D.S. Bhaskara Raju2, S.N. Pathuri2, K.V.S.S. Saikiran2, S. Sompalli2. 1Muhimbili National Hospital, Tanzania, 2CARE Hospital, Hyderabad-India. Correspondence to: Dr. EV Ussiri, CARE Hospital, Banjara Hills Road No.1, Hyderabad 500 034 India. E-mail address: eussiri@yahoo.com Code Number: js07033 Background: Anomalous pulmonary venous connection (APVC) is a rare, life threatening congenital heart disease presenting early in life. It may be partial (PAPVC) or total (TAPVC). PAPVC mainly involve the right pulmonary arteries and is associated with sinus venosus atrial septal defect with a low morbidity and mortality. TAPVC is classified into supracardiac, intracardiac, infracardiac and mixed types. It carries a high morbidity and mortality. The aim of this study was to determine the morphological patterns and surgical outcome of APVC at CARE hospital, Hyderabad-India. Introduction Anomalous Pulmonary Venous Connection (APVC) is one of the rare congenital heart diseases whereby, some or all of the pulmonary veins drain to the site other than left atrium1,2,3. Partial anomalous pulmonary venous connection (PAPVC) commonly involves the right pulmonary veins in more than 80% with normal drainage to the left side. About 90% of PAPVC are associated with Sinus Venosus Atrial Septal Defects - SVASD1,2,3. Total anomalous pulmonary venous connection (TAPVC) involves all four pulmonary veins which form a common pulmonary chamber and drain into different sites. It is classified according to the site of drainage as Supracardiac, intracardiac, infracardiac and mixed type as a combination of the mentioned types4,5. Definite diagnosis of APVC is made by Trans-Thoracic Echocardiography and Trans-Esophageal Echocardiography (TEE) and rarely, cardiac catheterization is used when associated with other cardiac anomalies or patient with age above 40 years to exclude coronary artery disease6,7,8. Clinical presentation and pathophysiology for PAPVC is similar to that of atrial septal defect (ASD) and the surgical treatment is directed towards closure of ASD while re-routing pulmonary veins into the left atrium using a patch. Surgical treatment carries a low morbidity and 0.9 % mortality rate3. TAPVC patients present with decompensated heart with desaturation and therefore, early presentation 9. Surgical treatment depends on the type of connection and this carries a high morbidity and mortality4,10,11 . A prospective study was done to determine the morphological pattern and operative outcome of the APVC at CARE Hospital, Hyderabad- India. Patients and Methods A prospective study was done from January 2004 to December 2006 including all patients who underwent cardiac surgery for anomalous pulmonary connection (drainage). Those patients whom their data could not be retrieved were excluded from the study. Operating theatre registry and medical record department were used to obtain the necessary details which included age, sex, type of anomaly and type of surgery done, number of veins and type of ASD involved in PAPVC, type of TAPVC and its associated anomalies, duration of mechanical ventilation. Also presence of pulmonary hypertension by echocardiography, pulmonary vein(s) obstruction and mortality were recorded. Preoperative and post-operative echocardiography was done for diagnosis and control respectively. All patients were followed up to the time of discharge for any immediate complication. Surgical techniqueAll patients with partial anomalies had glutaraldehyde treated pericardial patch closure of the ASD while re-routing pulmonary vein(s) into left atrium. Left pulmonary vein draining into innominate vein was divided and anastomozed to the left atrial appendage. All patients with supra-cardiac and infracardiac total anomalies had posterior approach whereby the common pulmonary venous chamber was widely (more than 4 cm) anastomozed to the left atrium to prevent obstruction. All patients with intra-cardiac anomalies underwent coronary sinus cut-back technique with glutaraldehyde pericardial patch closure of ASD while re-routing pulmonary venous blood into left atrium except one who underwent Van Praagh technique. All patients were started on cardiac support infusions; Milrinone (5-10µg/kg/min) and Dobutamine (2-20µg/kg/min) intraoperatively and transferred to Cardiothoracic ICU for elective ventilation, cardiac support and monitoring. ResultsThe study included a total of 65 patients whereby male accounted for 56.9% and female 43.1% (Table 1). Total anomalies were found in 39 patients accounting for 60% and 26 patients (40%) with partial anomalies (Tables 2 & 3). Mean age of presentation was 21.6 months (variance = 832.71, SD=28.86) for TAPVC and 135.2 months (variance = 27567.36, SD=166.03) for PAPVC (p = 0.0031). Among patients with partial anomalies 17 (65.4%) had involvement of one pulmonary vein (right superior pulmonary vein), 8 (30.8%) had involvement of two veins (right superior and right inferior pulmonary veins) and only 1 patient (3.8%) had involvement of three pulmonary veins (two from right side and one from left side draining into innominate vein ). Majority of partial anomalies were associated with sinus venosus ASD (84.6%) and only 7.7% were associated with posterior ASD and 7.7% ostium secundum ASD (Table 2). Among all patients with TAPVC 17 (43.6%) had supra-cardiac type, 14 (35.9%) had intracardiac type, 2 (5.1%) had infra-cardiac type and 6 (15.4%) had a mixed type (Table 3). TAPVC was associated with ostium secundum ASD in 20 patients accounting for 51.3%. Other rare anomalies associated with TAPVC included LSVC, PDA and VSD (Table 4). Pulmonary hypertension was found in 29 out of 39 (74.4%) patients with TAPVC compared to 3 out of 26 (11.5%) patients with PAPVC (X2 = 24.63, p=0.000001).There were 6 deaths from TAPVC group compared to none from PAPVC. All deaths were associated with severe pulmonary hypertension and 5 out of 6 were 2 months old. These deaths occurred within 48 hours of surgery except one that occurred on the seventh day and these were due to multiple organ failure due to low cardiac output syndrome and severe pulmonary hypertension. No patient reported to have post-operative pulmonary vein obstruction. Table 1. Age / Sex Distribution.
Table 2. Type of ASD associated with PAPVC
Table 3. Type of TAPVC
Table 4. Anomalies associated with TAPVC
Thirteen patients (33.3%) had no associated anomalies. DiscussionAnomalous Pulmonary Venous Connection present early in life. Lamb RK et al12) studied on APVC and found that 87.5% of all patients were less than 1 year old at time of operation. Our study revealed that 46.2% of all patients were 1-year old or less and TAPVC presenting early in life than PAPVC (mean age, 21.6 versus 135.2 months respectively, p = 0.0031). Male prepondence has been found in many studies1,7,12,13 as well as in our study. TAPVC occurs most common than the PAPVC. Snellen HA et al (1) studied on the patterns of APVC and found that TAPVC was 10 times more common than PAPVC. PAPVC mainly involves right pulmonary vein(s) and commonly associated with sinus venosus ASD1,3. NM Ammash et al6 while studying on the diagnosis of the PAPVC found that 81.4 % of the patients involved right pulmonary veins, 16.3 % involved left side and 2.3% was bilateral. CHA Jost et al3 when evaluating a long term post-operative outcome for 115 patients with sinus venosus ASD found that 97% were associated with APVC. Our study revealed that TAPVC accounts for 60% of all patients compared to 40% for PAPVC and among all patients with PAPVC 96.2% involved the right pulmonary veins. Supra-cardiac and intra-cardiac types of TAPVC are the commonest both accounting for 69.5% to 89.7% 4,10,12,13 which is comparable with our findings of 79.5%. Infra-cardiac and mixed types accounts for 10.0% to 31.3% and 20.5% in our study. Definitive diagnosis for APVC is mainly made by Trans-Thoracic Echocardiography (TTE) and Trans-Esophageal Echocardiography (TEE) is considered for sinus venosus ASD or unexplained dilated right side of the heart by TTE6,7,8. PAPVC carries a low morbidity and mortality of less than 0.9% compared to TAPVC which carries a mortality of 7 to 31%4,5,10,11,12,13,14, 15. TAPVC commonly is associated with ASD13 and when associated with a complex intracardiac anomaly the mortality increases to 52%16.The commonest anomaly associated with TAPVC in our study is ASD accounting for 51.3%. Overall mortality rate from our study was 9.2%; all deaths from TAPVC group making a mortality of 15.4% for TAPVC group. Pulmonary hypertension occured significantly in patients with TAPVC compared to PAPVC (X2 = 24.63, p=0.000001) and subsequently prolonged duration of mechanical ventilation and ICU stay. Mortality in our study was attributed to pulmonary hypertension and low cardiac output syndrome. Choudhary et al 4 found that the predictors for early death in TAPVC included young age at operation, need for emergency surgery, malnutrition, pulmonary vein obstruction, pulmonary hypertension and low cardiac output syndrome. There was no patient who developed pulmonary vein obstruction or cardiac arrhythmias in our study. Prevalence of pulmonary vein obstruction has been reported in other studies ranging from 6% to 14% occurring between 2 to 12 weeks or longer following surgery for TAPVC12,13,14,15. Pulmonary vein obstruction carries a high morbidity and mortality of more than 27% for re-operation15. Cardiac arrhythmias occurs very late following surgery for TAPVC and therefore a long term follow-up for these patients is recommended even when asymptomatic11,17. ConclusionTAPVC commonly present early in life and is associated with ASD and pulmonary hypertension. It carries a high morbidity and mortality. Accurate diagnosis and early surgical correction improves the surgical outcome. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07033t3.jpg] [js07033t2.jpg] [js07033t1.jpg] [js07033t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}