 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
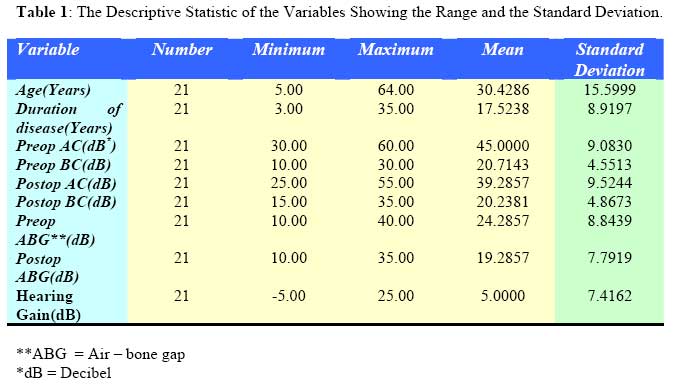
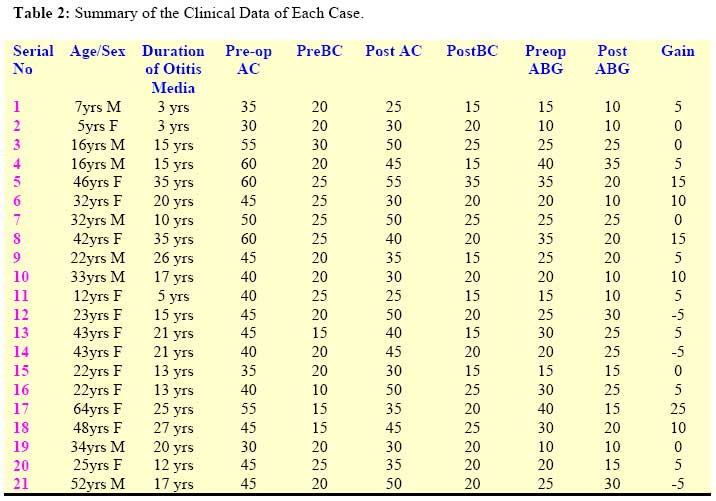
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 44-47 Hearing Outcome after Canal Wall down Mastoidectomy and Wullstein Type III Tympanoplasty Akeem O Lasisi MBChB, FWACS, FMCORL Code Number: js07038 Objective: This is to report the hearing outcome in patients who had CSOM, with ossicular erosion, treated with Canal Wall – Down Tympanomastoidectomy and the classical Wullstein type III tympanoplasty (CWDT) in which the graft was applied directly on the stapes footplate. Introduction Canal wall down mastoidectomy and tympanoplasty (CWDT) for complicated chronic suppurative otitis media is a common otological surgery particularly in the developing countries, despite this; reports of hearing outcome are few1. The aims of surgery are removal of the disease and preservation of a good hearing function, although the choice of the technique still remains a matter of controversy among otologists. The trend now is between canal-wall-down tympanoplasties and canal-wall-up tympanoplasty1, 2, 3, although the canal-wall-down tympanoplasties are more widely performed for cholesteatoma and chronic suppurative otitis media, with the merit that recurrences are reduced and the hearing outcome is not sacrificed4 - 6 . However, in cases with post – operative hearing loss, further treatment may involve the use of biologic and synthetic materials to reconstruct the ossicular chain and restore the transmission of sound3 - 7 . Our aim is to report the hearing outcome of patients with CSOM, complicated with malleus and/or erosion incus, who had mastoidectomy with the classical Wullstein type III tympanoplasty in which the fascia graft was applied directly on the superstructure of the stapes. Patients and Methods This was a retrospective review of hearing gain in patients who had surgery for CSOM with partial or complete erosion of the malleus and incus, exposing the stapes superstructure. The patients were offered modified radical or canal wall-down (CWD) tympanomastoidectomy and direct type III tympanoplasty where the fascia graft was applied directly on the superstructure of the stapes supported with gel foam or surgicel to maintain contact between the stapes footplate and the tympanic membrane graft. All the procedures were done under general anaesthesia using an operating microscope and the deep temporalis fascia was the source of graft. The in-patient chart of the patients managed in the hospital through 2004 to 2007 were retrieved and reviewed for biodata, clinical features and preand post-operative audiometry. All the patients had audiometry done with a computer audiometer BA 20 Kamplex in the sound - proof (acoustic) booth in the ENT clinic. Calibration: SO/DP 389 - 1983. The hearing was tested at the frequencies 250 - 8000Hz for each ear separately. The results were evaluated according to the guidelines of the Committee on Hearing and Equilibrium of the American Academy of Otolaryngology Head and Neck Surgery (AAO-HNS). Pure-tone average (PTA) was calculated as the mean of 0.5, 1, 2 and 3 KHz thresholds. Post-operative hearing gain was calculated from the air – bone gap before the operation and at the last follow-up examination. The duration of follow – up was between 18 to 24 months. The data were analysed with simple statistics and the correlation was found between the duration of CSOM and pre-operative pure tone average. Results A total number of 21 canal – wall Down tympanomastoidectomy (CWD) and type III tympanoplasty (myringostapedioplexy) were done involving 13 females and 8 males aged between 5 and 64 years, mean 30(SD = 15.59). All the patients had CSOM with mastoid abscess and partial or complete erosion of the malleus and incus and intact footplate of the stapes. Foreign body was seen in the middle ear of patient 2, middle ear polyp in 6 – 11 and meningitis and destruction of the tegmen tympani in 3, 4 and 5. The duration of otitis media was 3 – 35 years, mean 17.5(SD = 8.9) and there was correlation with pre-operative air conduction pure tone average (r =0.580, P = 0.006) and pre-operative air- bone gap(r = 0.610, P = 0.003). The mean hearing gain was 5dB (with a range between -5 and 25dB), and hearing gain between 10 – 25dB was achieved in 5/21(24%).The pre-operative Air conduction (AC) pure tone average (PTA) was 30 – 60dB, mean 45dB (SD = 9.08) and BC PTA ranged between 10 and 30dB, mean of 20.7 dB(SD = 4.55). While the postoperative AC was between 25 and 55dB, mean of 39.29(SD = 9.5), the BC was between 15 and 35dB, mean of 20.23(SD = 4.9). The preoperative air – bone gap (ABG) was between 10 and 40dB, mean of 24.29(SD = 8.8) while post-surgery it was between 10 and 35dB, mean of 19.29(SD = 7.8), table 1. Summary of the patient is in table 2. Discussion Reports of hearing outcome after CWDT are few despite its widespread use8 - 10 . We used this modified radical mastoidectomy combined with type III tympanoplasty with the goal of achieving control of disease and correcting hearing loss. Artuso et al8 reported an improvement from the mean preoperative ABG of 28.44 dB to 24.06 dB in a two years after a Wullstein surgery for cholesteatoma. This is comparable with our finding of 24.29 and 19.9 dB for pre – and post– operative ABG. However in our review, only 5/21 gained significantly useful hearing. This may further support the need for further hearing augmentation surgery in these patients. According to reports, patients with ossiculoplasty showed significant hearing improvement compared to direct type Wullstein’s tympanoplasty8,9 . This is also supported by Vartiaine who reported a mean hearing gain of 10.8 dB and closure of the postoperative air-bone gap to within 20 dB in 51% of 277 6 years after ossiculoplasty and tympanoplasty. In our report the mean hearing gain is 5dB which may not be significant to the patient. The present findings show that autologous ossicle and cortical bone are still suitable for ossicular reconstruction in chronic ears, especially when one-stage surgery is preferred. Shinohara et al10 also reported success in hearing in 46 – 68 % of 65 patient between 1- 2year after an ossiculoplasty. However, they also reported extrusion of the prosthesis in 17 ears (16%) with a mean postoperative period of 27.7 months. Besides this complication, the non-availability of implants in our own environment remains a major obstacle in our patients. The other is the inability to afford a second look surgery which may be expedient in the management of the patients. Staging of tympanoplasty has been found to be important in management of mucous membrane problems in severely diseased ears11 . In a review of 400 staged cases over a 3 year period, Shelton and Sheehy11 reported that almost one third of cases with middle ear cholesteatoma at the first stage had residual disease on reexploration; advanced disease due to late presentation which are common in our patient population is a further indication for staging tympanoplasty. This is confirmed by finding of positive correlation between duration of disease and the preoperative air-bone gap and AC pure tone average. In contrast, MacAndie and O'Reilly12 did not find any correlation between the duration of disease and hearing loss in their report. They also reported that the presence of cholesteatoma and ossicular erosion was not associated with a significantly increased risk of sensorineural hearing loss. The elevated bone conduction threshold found in our patient is thought to be due to associated labyrinthitis most likely toxic variety which follows longstanding chronic CSOM. In addition a postoperative depression of bone conduction seen in 4 cases (5, 16, 17, 18) were attributed to otologic trauma due to the vibratory effect of the electric drill on the cochlear labyrinth. The other factors that may further contribute to AC loss in our patients may be persistence of disease in the mucosa, tubal malfunction, ossicular erosion and fibrosis of the ossicular joints and middle ear. Our impression is that these patients may benefit from an ossiculoplasty, or the use of a hearing aid or bone – anchored hearing aid (BAHA). These devices are generally expensive limiting access, access to hearing aid has been reported to be about 12.5%13 of the patients while BAHA and ossicular implants not yet available in most parts of the sub-Saharan Africa. However, significant hearing benefit has been reported with their use. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07038t2.jpg] [js07038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}