 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
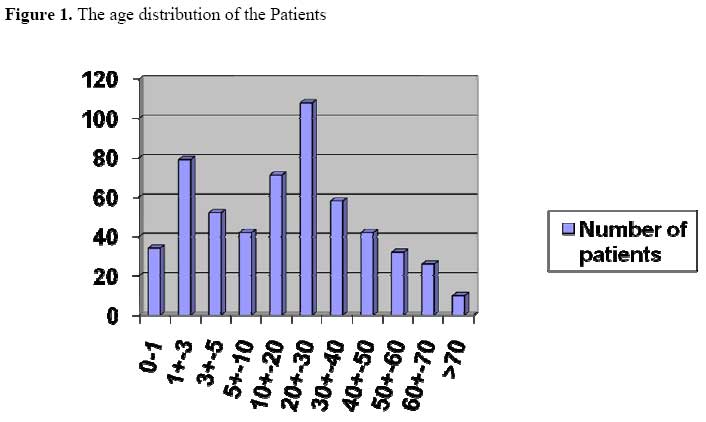
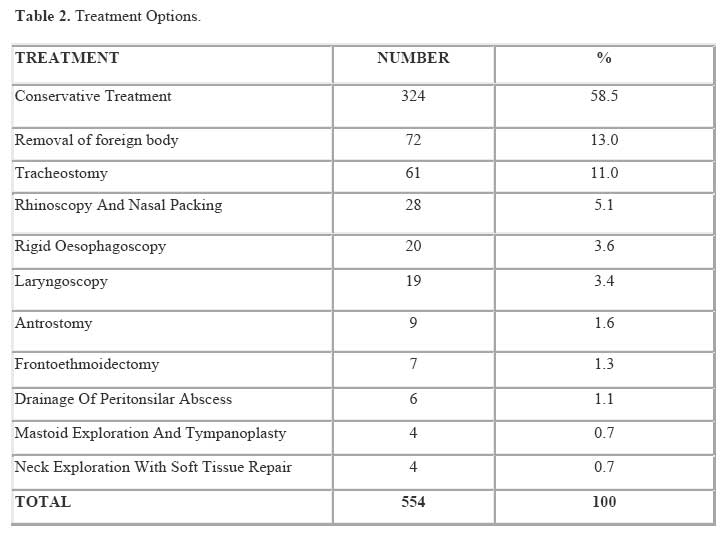
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 48-52 Otorhinolaryngologic Emergencies In Nigeria, Sub-Saharan Africa: Implication for Training. O.A. Lasisi1, Z.K. Imam2, A.A. Adeosun1 Code Number: js07039 Background: The anatomy and function of the ear, nose and throat (ENT) make pathologies potentially catastrophic. Reports on the epidemiology of otolaryngologic emergencies put the prevalence at between 30 and 80%. There are however very few studies from the developing countries. This study was aimed at determining the magnitude and spectrum of otolaryngologic emergencies in a teaching hospital in a developing country in sub-Saharan Africa.. Introduction The proximity to the brain and presence of the airway in the region of the ear, nose and throat makes pathologic processes potentially catastrophic. Swift recognition and prompt institution of management becomes crucial to successful outcome. In the United state, otorhinolaryngologic emergencies are reported to represent between 30% and 80% of presentations seen by emergency department physicians1,2. There have been few reports on the epidemiology of otolaryngologic emergencies especially in the developing countries, despite their apparent increasing tendency. We report the epidemiology and management of the emergencies and discuss the implication for medical curriculum in Nigeria. Patients and Methods This was a retrospective study of the total number of ENT cases referred during call - duty hours or managed as emergency cases between July 2001 and 30th June 2003 inclusive. The clinical records were reviewed and the biodata, diagnosis and treatment were extracted. We included all the cases of vital emergencies needing immediate intervention to save life and urgent cases needing intervention for control of pain, bleeding and drainage of abscesses. The data was analysed using Microsoft excel, and the results are presented in pictorial forms. Results The emergency cases accounted for 554 (21.8%) of 2,544 patients seen in the Otorhinolaryngology Department in the period under study. Of these, 316 (57%) were males and 238 (43%) were females. Their ages ranged between 4 months and 80 years with peak in the third decade. The paediatric age group (0- 14years) constituted 237(42.8%) of the cases (Figure 1). General practitioners referred 459 (83%) of the cases and 95 (17%) were referred by Paediatricians. Recurrent otitis media accounted for 134 (24%) cases, followed by foreign bodies in the orifices in 119 (21%) of cases. Head and neck trauma accounted for 111 (20%), epistaxis for 88 (16%) and chronic rhinosinusitis for 29 (5%) of the cases case. The findings are summarized in Table 1. Conservative management was offered in 324 (58.5%%) of the patients. Surgical procedures required included removal of foreign body from the ear in 72 (13%), tracheostomy in 61 (11.0%), rhinoscopy and nasal packing in 28 (5.1%) and rigid oesophagoscopy in 20 (3.6%) of the cases. These results are summarized in Table 2. DiscussionEmergency cases constituted 22% of otorhinolaryngologic workload in our center; this is similar to the report of Sorensen3. The top five were recurrent otitis media, foreign bodies, head and neck trauma, epistaxis and chronic rhinosinusitis. This was comparable to findings by workers4,5 . Palchun et al4 reported acute otitis externa and chronic otitis media to be commonest in a study of 580 emergencies. However, there is a slight variation from the report of Huang et al6. In their series, out of 2561 cases reviewed, the top five were epistaxis (22.7%), foreign body in the throat (18.7%), acute tonsillitis (11.4%), acute otitis media (7.7%) and foreign body in the ear in 6.4%. The preponderance of acute otitis media in our study further confirms its high prevalence. This may be due to a number of predisposing factors such as poverty, malnutrition, over crowding and delayed presentation. Severe otalgia and the danger of intracranial or systemic spread of infection constitute the basis of emergency intervention. The complications encountered were acute mastoid abscess, meningitis and brain abscess. Our study confirmed what Hon et al7 reported that the ear is the most common site for foreign body, making removal of foreign body from the ear the commonest ENT surgical procedure. Epistaxis was commonly idiopathic, usually mild to moderate and was controlled by nasal packing, except in a few cases in which it was severe and necessitated blood transfusion; and external carotid ligation was done once. The complications of chronic sinusitis resulting in emergency consultation were mainly orbital abscess with sepsis, mucocoeles and cavernous sinus thrombosis. Airway obstruction constituted the emergency in foreign bodies, tumours, trauma of the laryngotrachea and acute neck abscesses necessitating tracheostomy. Besides foreign body removal from the ear, it is the most common emergency procedure. The trauma cases were found in the third and fourth decade of life, the active economic force, upper airway obstruction constitute the indication for emergency. A mortality rate of 20% was reported in head and neck injuries1,2. This was attributed to damage to vascular structures, cervical spine, oedema and laceration of the laryngotrachea cartilage, fracture of floor of the mouth and excessive bleeding with aspiration1, 2. However, all the neonates with laryngomalacia were managed conservatively. This study confirmed the preponderance of paediatric population in otolaryngologic emergencies. Furthermore, all the patients had earlier been managed by general medical practitioners and paediatricians before referral to the otolaryngologist, despite only about 55% needing surgical intervention. In addition, all the children with laryngomalacia were managed conservatively. This suggests that a high proportion of these cases could have been managed by the referring physicians with appropriate conservative treatment. The principles of management include airway maintenance and oxygen administration, control of epistaxis, analgesics, antibiotics therapy, and use of anti-inflammatory drugs. However, this requires appropriate knowledge and skill in the management which is related to training. The present training of general practice specialists involves a one month exposure in ENT out of 60 – 72 months. It is our strong opinion that the duration of Otorhinolaryngology exposure should be increased with more intensive practical training of general practice. This is expected to improve management of common ENT cases and proper patient selection for referral, so that only the real emergencies References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07039f1.jpg] [js07039t2.jpg] [js07039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}