 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 62-71 Non-operative Ambulatory Treatment Osteonecrosis of the Femoral Head in Sickle Cell Disease E.K. Naddumba MMed (MU), FCS (ECSA) Senior Consultant Orthopedic Surgeon, Mulago Hospital – Kampala Uganda. Code Number: js07042 Osteonecrosis of the femoral head of the femur (ONFH) is a common disabling complication in Sickle cell Disease (SCD). Sickle cell disorder include patients homozygous for hemoglobin S (HbSS) patients with sickle cell c (Hbsc) disease, those with sickle cell beta thalsaemia, and those who have other rare conditions in which Hbs is combined with abnormal beta globulin chains. ONFH in SCD is a result of erythroid hyperplasia or thrombosis and infarction. This stiff cells obliterate the microcirculation to the femoral head. The prognosis of ONFH in SCD depends on the age of the patient and the severity of involvement of the femoral head. It is characterized by pain in the hip without radiological sign during the early stage of the disease. Specific features in late disease include small cysts, diffuse osteoporosis, subchondral osteoporosis/sclerosis, and a mixed osteoporosis/sclerosis. This stage last several months. Early diagnosis of ONFH increases the chances of treatment success. Plain X-rays are useful for late stage disease. Magnetic Resonance Imaging (MRI) is the most sensitive for diagnosing ONFH in the early stages. Treatment of ONFH in SCD depends on the stage of the disease. Surgical options include Core decompression, femoral osteotomy, pelvic osteotomy, hip arthrodesis, and total hip replacement arthroplaasty (THA). THA is indicated when the femoral head has collapsed and with arthritic changes. In this case series, short results on non-operative ambulatory treatment are presented.Introduction Osteonecrosis of the femoral head of the femur (ONFH) is a common disabling complication in Sickle cell Disease (SCD). At Mulago Hospital, the prevalence of ONFH among the sicklers is 21.3%, and the mean onset of symptoms is 14.9yrs1 . This complication in SCD usually starts in young adolescents and is rare below the age of 6 to 7 years2 . The prevalence of the disease is between19% and 31%6 . Bilateral hip disease occurs in 54% of cases3 . Sickle cell disease is a congenital chronic unrelenting persistent hemolytic anemia4 . And is the most common severe inherited disease on the African continent5 . It is a haemoglobinopathy characterized by the inheritance of 2 abnormal genes of hemoglobin, at least one of which is the sickle cell gene. It results from an abnormality of the Beta globulin gene on chromosome 11 that causes substitution of Valine for Glutamic acid at the 6th codon from the amino acid terminus19. It is inherited as an autosomal recessive manner. Sickle cell disorder include patients homozygous for hemoglobin S (HbSS) patients with sickle cell c (Hbsc) disease, those with sickle cell beta thalsaemia, and those who have other rare conditions in which Hbs is combined with abnormal beta globulin chains Its incidence ranges between 5% to 40%3 . Sickle cell syndromes are common in Geographical areas where Malaria is Endemic. The genes have the highest incidences in Africans, Arabs, Mediterranean Countries and Asiatic Indians6 . ONFH in SCD is a result of erythroid hyperplasia or thrombosis and infarction. In SCD, the main change in blood, which causes osteonecrosis, is the diminished deformability of the red blood cells as the HbS molecules polymerize into rigid aggregates due to low oxygen tension (hypoxia). Under this conditions, the originally disc shaped red blood cells become less deformable and assume a sickle shape. This stiff cells obliterate the microcirculation to the femoral head. Sickling of red blood cells in the microcirculation of bone results in intramedullary sledging, stasis, thrombosis, and destruction of the vessel walls, edema and progressive ischemia7,8 . In Sickle cell trait, (HbAS) the concentration of HbS is not as in SCA, therefore sickling is much less common and bone infarction is very uncommon9. Nevertheless it is a hazard under certain conditions eg.high altitude, anaethesia, extreme cold, and airplanes10. There are mechanical factors involved in the production of ONFH, This is obvious from the fact the necrotic zone is situated around the upper pole of the femoral head and that the collapse of the femoral head always occurs at the weight bearing region3. The prognosis of ONFH in SCD depends on the age of the patient and the severity of involvement of the femoral head. Young patients have a reasonable potential for healing of ONFH, while the young adolescent with total involvement have a poor prognosis. The natural history of disease progression can be staged according to the Arlet and Ficar 11 System although it may not be specific for SCD: Stage I: This is the pre-radiological stage characterized by a total absence of radiological features. It is characterized by pain in the hip without radiological sign. The chief complaint of the patient with ONFH is usually localized pain in the groin, but occasionally to the ipisilateral buttock and the knee. There is associated tenderness and limited movement with active and passive range of motion especially with internal hip rotation. Early diagnosis of ONFH increases the chances of treatment success. Plain X-rays are useful for late stage disease. Magnetic Resonance Imaging (MRI) is the most sensitive for diagnosing ONFH in the early stages. CT scan is less sensitive than MRI, but can be used to detect the extent of the bone damage. Bone scan with the use of Technetium 99 m diphosphonate has the potential for diagnosing ONFH before irreversible changes are visible in routine roentgenograms12. Treatment of ONFH in SCD depends on the stage of the disease. Options include Bed rest, skin traction, non-weight bearing, bracing, and physiotherapy. Ambulatory treatment with the use of a walker/crutches and nonweight bearing can help manage the pain while at the same time protect the joint until surgery. Surgical options include Core decompression, femoral osteotomy, pelvic osteotomy, hip arthrodesis, and total hip replacement arthroplaasty (THA). None of these procedures have proved to provide the best solution. THA is indicated when the femoral head has collapsed and with arthritic changes. The long-term durability of THA in ONFH is typically not as good as it is in arthritic hips. In this presentation, shortterm results of ambulatory non-operative treatment are presented with a purpose of recommending this method in non-arthritic hips due to ONFH in SCD, which can be salvaged and possibly avoid Joint replacement Arthroplasty procedures. Patients and MethodsA series of 16 known sicklers with painful hips were referred to the orthopedic department from the SCD Clinic at Mulago Hospital during the year 2004,for further management.15 of them were confirmed HBSS and 1 was HBAS.Non had received treatment for their painful hips. The 1st pelvic radiographs were taken after clinical assessment to confirm the diagnosis. Other diagnostic investigations like Bone Scan in the early stages and MRI were not done due to unavailability. CT Scan was also not requested because of costs. The average age of the patients was 15.5 yrs, 14 of the patients were males and 2 were females. All the patients presented with pain in the groin of the affected hip joint radiating to the ipsilateral knee joint. They all had a painful limp, restricted and tender passive internal hip rotation and a positive FABERE Test (Flexion, Abduction, and External Rotation passive movement). Three of the patients had a right hip involvement, 10 had left and 3 had bilateral involvement. The duration of the symptoms was 2weeks to 19yrs; the majority presenting within 5 months of onset of the symptoms. After confirmation of the diagnosis, nonoperative ambulatory treatment as outpatients was prescribed to all the patients. This involved crutch walking with a pair of elbow crutches. Physiotherapy was prescribed for hip exercises, and muscular strengthening of atrophic groups of hip and quadriceps muscles. Prophylactics Antibiotics (Ciprofloxacillin) and analgesics (Diclofenac) were also prescribed during the acute painful phase. Patients were encouraged to take plenty of oral fluids, weekly antmalarials (chloroquin), and folic acid. They were all reviewed on a monthly basis in the outpatient clinic, and follow up radiographs at 6 monthly intervals. During follow up they were monitored for pain response on treatment, improvement of range of motion in the affected hips, and evidence of healing of the lesion by revascularization. Consideration to discontinue the crutches was done when pain had subsided and radiological confirmation of evidence of healing of the osteonecrosis by revascularization. They were then recommended to continue with a simple walking stick. ResultsRadiological staging: The majority of the patients presented with stage II disease (Table 1) Duration of TreatmentThe average treatment with crutches was 12months, with a minimum of 5months and a maximum of 18 months. Response to TreatmentAll the patients had their pain controlled, regained hip motion, and x-rays showed evidence of healing of the lesions. Case reportsDML: Was a 16-year-old male known sickler who presented with bilateral Hip pain that had lasted 10 weeks. The symptoms started with the right hip joint and a month later the left hip was also involved. On examination, he had a tinge of jaundice, had mild to moderate anemia, and had no temperature. He walked in the clinic being supported by the mother because of pain in the hips. Both hips were tender and had Table 1. Stage of Disease on presentation
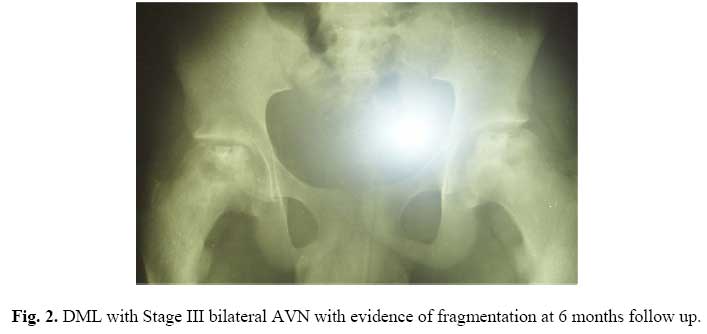
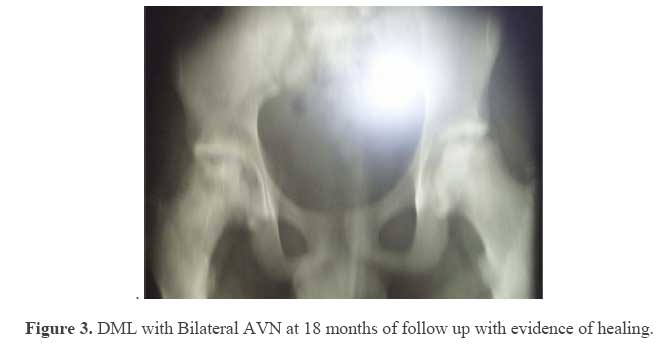
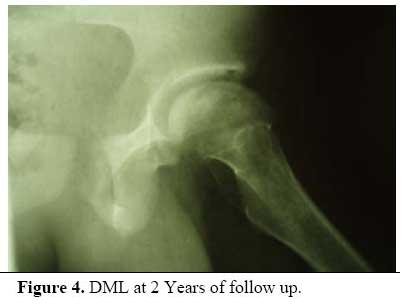
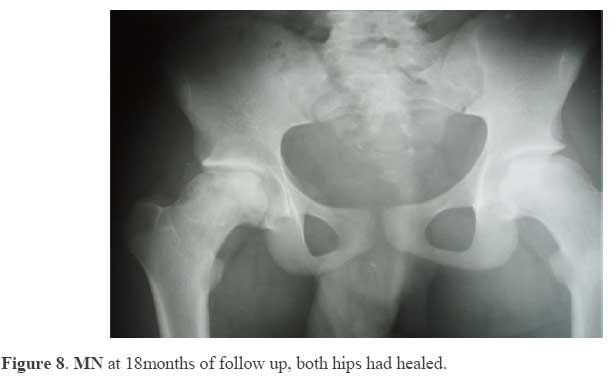
Figure 1. DML with AVN Stage 11 on the left and Stage 111 on the right hip. significant restriction of passive internal rotation both hips. X-rays of the pelvis was requested and the results are shown in figure 1. He was put on prophylactic antibiotics, analgesics, folic acid, plenty of oral fluids, At 6 months pain had subsided range of hip motion had improved but was recommended to continue with crutch walking. Check Xrays done at 6 months of follow up are shown in Figure 2. At one year of follow up, there was no pain in both hips. Had normal range of passive and active hip motion. He was recommended to continue with the pair of elbow crutches for another 6 months. X-rays done at 18 months of follow up are shown in Figure 3. At this stage crutches were discontinued but recommended a weekly chloroquin, and prescribed crutch walking with a pair of elbow crutches. Physiotherapy was also prescribed. He was managed as an outpatient and reviewed monthly in the out patient clinic. walking stick. At 2yrs of follow up, the pain had completely improved in both hips. He was able to ambulate with a normal gait without pain and no limp. He had regained normal range of hip motion, both passive and active movements. Check x-rays are shown below in figure 4 and 5.At this stage he was still recommended to continue ambulation with one elbow crutch and hip exercises, and to be reviewed after 6 months. MN was a 16-year old male sickler who presented with bilateral hip pain that had lasted for over a year. The pain was more marked in the left hip joint. He had limitation of internal rotation both hips due to pain. Xrays done on the first visit showed late stage III disease both hips (Figure 6). He was prescribed physiotherapy, analgesics, weekly chloroquine, folic acid and a pair of elbow crutches for ambulation. Follow up was done at monthly intervals. Three months later he was noted to be making a steady improvement. X-rays done at one year of follow up are shown in Figure 7. At 18 months of follow up the patient had improved. Crutches were discontinued. Copies of X-rays at this stage are shown in Figure 8. TM was a 14-year-old male, referred from the SCD Clinic, with painful right hip joint. His haemoglobin electrophoresis was SS. He had a painful limp and restriction of internal rotation of his hip. Rays of his pelvis showed a collapsed super lateral surface of the femoral head right hip joint, and a subchondral fracture (Figure 9) Stage 111 disease. He was started on crutch walking, and 6 months later, he was noted to be improving, with less pain in the hip joint and improved range of hip motion. Check x-rays showed a collapsed flattened superolateral surface of the femoral head and evidence of patchy osteoporosis, a sign of revascularization (Figure 10). He was recommended to continue with crutches. At 12 months, pain had subsided completely, and walked with a positive Trendenburg gait. Passive and active range of hip motion had been restored to normal, and check x-rays showed evidence of fragmentation, (Figure 11) but remained deformed. He was recommended to change to a walking stick DiscussionOsteonecrosis of the femoral Head in patients with Sickle cell disease is associated with progressive chronic pain in the affected hip joint with resultant severe disability in the lower extremity. The natural history of the disease is progressive distraction of the femoral head with massive necrosis, which may begin with a small portion of the head often the postero lateral surface and may progress to involve the entire head. The disease may be bilateral in some cases hence causing severe ambulatory disability. In the very young patients with osteonecrosis due to Sickle cell disease, healing of the lesion occurs as in Legg Calve Perthes disease because of revascularization, however teenagers or adolescents may not have the potential for revascularization hence progress to massive necrosis, femoral head distraction and permanent disability13. The treatment of osteonecrisis in Sickle cell disease has been addressed by several authors13. Conservative methods include Bed Rest, Non- Weight Bearing, Bracing and Physiotherapy. Almost all involved joints in the lower extremity respond to Non-weight bearing measures, which include bed rest, traction for acute pain, crutch walking, and bracing. Blood transfusion is believed to promote healing of the necrotic lesion by reducing sickling. In pre-adolescents, Abductor Braces similar to those used in Legg Calve Perthes disease may prevent further collapse by redistributing the compressive forces to the lateral intact portion of the femoral head. Crutch walking requires follow up for at least one year to ensure that gradual collapse of the femoral head has ceased to progress during revascularization. Physiotherapy is essential for strengthening the hip abductors, adductors and hip extensors that normally undergo disuse atrophy due to the chronic hip pain. It also preserves hip motion. Suggested surgical options include proximal femoral varus osteotomy to redirect the femoral head in the acetabulum, remove compressive forces from the necrotic zone, and allow healing of the lesion by revascularization. Other surgical options include adductor tenotomies followed by broom stick abduction plaster cylinder to allow adequate coverage of the femoral head in the very young, Chiari pelvic Osteotomy in the teenagers, Cup arthroplasty, metal prosthesis (Hemiarthroplasty), Total hip replacement arthroplasty, and arthrodesis. The failure rate following surgical treatment by prosthetic replacement arthroplasty is 50% at 5.4years follow up14. Surgical risks include cardio vascular complications, infection, implant and loosening. Arthrodesis has limited use because of the fear of opposite hip avascular necrosis development. In this case series, Operative Ambulatory Treatment (crutch walking) was prescribed to young adolescent sicklers who presented with avascular necrosis (Stages I - III) disease. Pain control, improved range of motion and evidence of revascularization were observed after a period of 18 months of follow up. Although the cases are too few and the period of follow short, the results so far seem promising. Conclusion and RecommendationIn this case series, promising results have been observed. Ambulatory treatment with use of crutches can help in management of the pain associated with osteonecrisis of the femoral head in sickle cell while at the same time protecting the hip joint from further. This non-operative treatment method may be a solution to early stage AVN in sickle cell disease and hence protect these hips from surgical options. A Prospective study involving a larger series of cases with a longer follow up period and detailed investigations with MRI/Bone Scan is recommended before a definitive conclusion and recommendation are made. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07042f9.jpg] [js07042t1.jpg] [js07042f6.jpg] [js07042f4.jpg] [js07042f2.jpg] [js07042f8.jpg] [js07042f5.jpg] [js07042f10.jpg] [js07042f7.jpg] [js07042f3.jpg] [js07042f1.jpg] [js07042f11.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}