 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 72-76 Management of Segmental Tibial Fractures. N. S. Motsitsi
Code Number: js07043 Segmental tibial fractures are uncommon injuries that occur in about 12.8% of tibialfractures. They are commonly caused by high-energy trauma. It is estimated thatalmost 50% of these fractures are open. They are often part of multiple injuries. They are challenging to manage and have a significant complication rate. Literature search retrieved very few articles (10) on the management of segmental tibial fractures. There has been a significant change in the management of these injuries. This has been made possible by the development of new Orthopaedic implants. Three currently favored methods of treatment are intramedullary locking nail , external Fixators (with their different constructs and versatility) and Plaster of Paris. It is important to note that more than two-thirds of segmental tibial fractures will require more than one surgical intervention. The surgeon therefore, needs to plan ahead to make subsequent surgical interventions possible. There are no clear therapeutically- relevant guidelines regarding classification of segmental tibial fractures , treatment approaches and evaluation of functional outcome using validated scales. These are the crucial issues or challenges facing future clinical research studies. Introduction A segmental fracture is defined as a fracture with two or more fracture lines with one or more cylindrical intercalary segment(s). The majority of segmental tibial fractures have one intercalary segment. These fractures are rarely encountered, accounting for only up about 12,8% of tibial fractures1 . They are caused by high-energy injuries; motorvehicle and motorcycle crashes, falls from a height, industrial and train accidents. Some are caused by low – energy injuries such as sports and twisting the leg. The incidence of open segmental fractures varies considerably from study to study ; it ranges from 37.5% to 83.8% 2,3, . Segmental tibial fractures are often part of multiple injuries. Segmental fractures are considered as a separate clinical entity from the normal tibial fractures for a number of reasons. These include:
The management of these fractures pose a formidable change to the treating surgeon. The number of available implants has escalated dramatically over the last decade , and the treating surgeon is simply overwhelmed by these implants and the new concepts and surgical techniques that accompany them. The important questions pertinent to the treating surgeon are the following :
This narrative review evaluates the available literature with a view of trying to find answers to these clinically relevant questions. Methods and Results. The methods and results used for literature survey are outlined below. A. Inclusion criteria.
C. Literature Search Strategy. Key words: segmental, tibia fracture(s).
All potentially relevant articles were individually reviewed. Ten articles were found to be relevant to the topic. All articles were descriptive studies. There was one prospective study and the rest were retrospective. DiscussionBoylston et al5 forty years ago reviewed 28 patients and outlined treatment options for segmental tibial fractures. The options were:
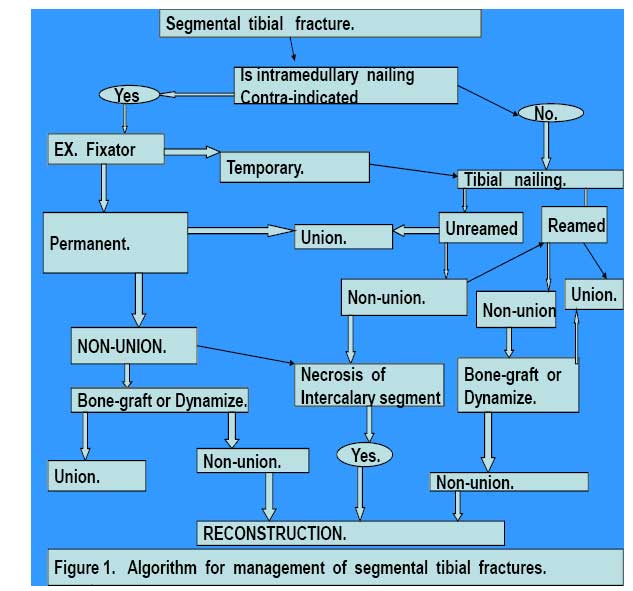
They followed their patients for an average of 26 months (12 -51 months). There were 2 non-unions ; one patient was treated with cast and the other with a plate. There were 13 patients with open fractures. It is not clear how patients were allocated. However, the methods laid the foundation for the management of segmental tibial fractures. The implants have improved over the years but the principles of treatment have not changed dramatically over these years. In 1969, Zucman and Maurer6 introduced the technique of unreamed tibial nailing in the management of both closed and open segmental fractures. There was no grading of open fractures as we know it today. They found that 19/36 ( 79%) of open fractures achieved union without complications. There were two cases of non – union of closed fractures. Deep sepsis developed in four cases (12%); two of these united without any surgical intervention. Tibial nailing was to be the major technique in the management of these fractures as will be evident in subsequent cases. Functional outcome of segmental tibial fractures was not documented in the majority of previous reports. Oivind and Olav7 reviewed 54 patients with the aim of documenting functional outcome . They found that 53.7% of their patients had full recovery and the rest had some form of functional impairment. Their assessment was to have great impact to subsequent authors: it was clear that closed segmental fractures should be viewed differently from open ones. It was Melis et al8 who, in their reviews of 38 patients separated the treatment of open and closed segmental tibial fractures. They used reamed K-nail -Hertzog nail. Open fractures were treated with antibiotics for 20 days plus continuous irrigation and suctioning for at least 10 days. Soft tissue coverage was done after 10 days. They clearly documented all complications which occurred that included skin breakdown, malunion and sepsis. They noted that skin breakdown did occur in closed fractures as well. Woll and Duwelius4 used Ender nails in both closed and open fractures. All fractures united. The few complications they encountered included superficial sepsis, DIC, shortening and malunion. Complications associated with non-locking nails were mal-union and shortening. It was becoming increasingly obvious to a large number of surgeons that segmental tibial fractures have a significant complication rate. Rommens, Coosemans and Broos9 reported in the experimental and clinical forum that in their 37 cases , they had a 70.2% complication rate. They stated that plating in these cases is dangerous and should not be done. They had double-plated 18 patients and obtained union in all. Their results showed that plating is safe. It is not clear as to what happened to their other patients. Selection of patients is crucial in theses fractures. Chiu-Chuan and Chun-Hsiung4 in their series, selected their patients carefully. They did locked intramedullary nailing in closed fractures and Grade 1 open fractures. They excluded Grades II and III fractures. Open fractures were treated with antibiotics for three days before nailing. All fractures except one united. One patient had insignificant malunion. Ching-Kuel et al10 in their 33 cases used a similar approach and obtained union in 32 (97% union rate). There was one case of non-union and two cases of deep sepsis. The non- union united after bone grafting. In a 2003 review of 27 cases by Giannoudis et al1, the treatment modalities in their units were unreamed tibial nailing in both closed and open fractures, external fixators (for open fractures), locking plates in closed fractures and P.O.P. for closed fractures. Antibiotics were given for five days in open fractures. A total of 48.1% required a second procedure while 18.5% required a third procedure. The complications included 1 non-union, deep sepsis, skin necrosis which occurred in both closed and open fractures, compartment syndrome in 11.5%, malunion, nonunion osteonecrosis of the intercalary segment, osteitis, delayed union and nonunion. Two cases had amputations. Giannoudis et al1 findings send a very important message that “66.6% of segmental tibial fractures require more than one surgical intervention”. It is therefore extremely vital to plan ahead so that should subsequent surgical interventions become necessary, the surgeon is well prepared for it. This The author of this review proposes the algorithm shown in FIGURE 1 for application in management of segmental tibial fractures. Conclusion The current literature offers very little in terms of the issues and questions raised at the beginning of this review. However , some principles or approaches are evident in the literature :
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07043f1.jpg] |
| |||||||||

{kind=link}