 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
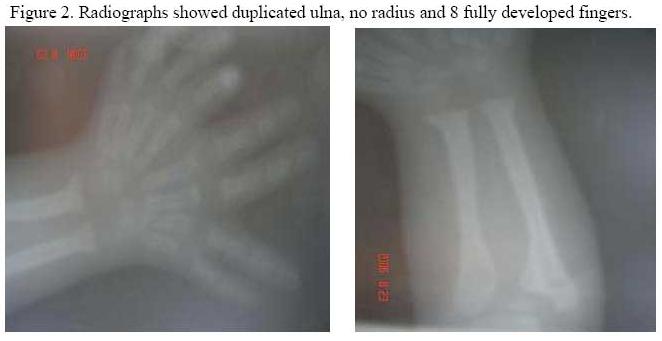
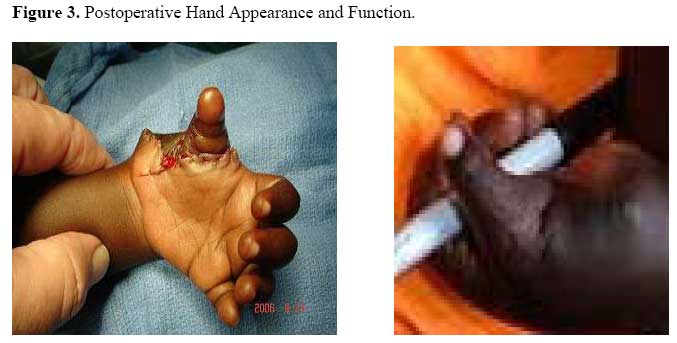
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 88-91 Mirror Hand (Ulna Dimelia): A Case Report. E.N. Muteti, L.L. Carter Code Number: js07046 This is a case report of ulnar dimelia (mirror hand). The literature review and a discussion of the classification systems of anomaly, variations, surgical techniques and the technique used in this patient are presented Case PresentationA 1-year 4months old baby girl was seen at the AIC-CURE International Children's Hospital, Kenya, born with eight digits in the left hand. She is the product of a nonconsanguinous marriage. Pregnancy, delivery and postnatal periods were uneventful. There is no one with multiple digits in the family. Examination revealed a normal baby girl without any other congenital anomalies apart from the left upper extremity. There was duplication of four fingers on the radial aspect of the hand and no thumb. The wrist movements were normal. The left forearm was shorter than the right forearm. Flexion of the elbow and supination/pronation of forearm were limited to 45 degrees and 10 degrees respectively. TreatmentDue to the mother’s serious concern about the grotesque appearance of the daughter’s, we decided to perform surgery. It was noted that the web space between the ulnar index finger and duplicated radial index finger was wider than for the others. The duplicated radial index finger was of adequate size, pronated about 35-45 degrees and with good flexion and extension; and suitable to be used for pollicization. The radial small, ring and long fingers were to be deleted. The incision was made along the thenar crease and around the base of the radial index finger. The three radial digits were filleted out. Radial digital vessel to the ulnar index digit was divided and ligated to allow pollicization of the radial index finger. A shortening osteotomy of the radial index metacarpal was done through the base and at the distal physis. The radial index digit was rotated 140 degrees and the distal epiphysis was volar flexed and fixed to the base of the proximal phalanx. The flexor tendon of the radial small finger was transferred to the radial index digit to become the abductor pollicis longus. The dorsal interosseous muscle was transferred to the proximal phalanx to become the abductor pollicis brevis and the volar interosseous became the adductor pollicis. Redundant skin was excised and incision closed around the base of the pollicized radial index in good thumb position. DiscussionMirror hand, also known as ulnar dimelia, is an extremely rare condition with reported incidence of 70 cases in the last 300 years. It is characterized by the presence of duplication of the ulna. There is no radius and almost symmetrical duplication of the ulna digits around a central digital axis producing seven or more digits. This patient had two ulna bones in the left forearm and eight fingers in the left hand. Anatomically, the carpus appears symmetric with a large lunate surrounded by triquetrals on either side. There are two capitates, two extensor tendons to the central digit and a duplicated ulna nerve. Arterial supply is through a lateral vessel supplying the radial two and a half digits and a medial vessel supplying the ulnar four and a half digits1 , 2. Variants of ulnar dimelia have been reported in literature3,4,5,6. These included patients with two ulnae and one radius, two radii and one ulnae; and ulna dimelia with other congenital malformations. A classification of the mirror hand-multiple hand spectrum has been proposed by Al-Qattan and Al-Thunayan et al7. The patients had multiple fingers in which: type 1 is ulnar dimelia (two ulnae), type 2 is intermediate with two ulnae and a radius, type 3 is intermediate with one radius and ulna, type 4 is syndromal mirror hand; and type 5 is multiple hand. The case we are presenting is type 1A in which the two ulnae are fully developed. Overall type 1 is the most common with type 1B being more commonly reported than type 1A. The embryology of mirror image was first described by Saunders and Gasseling, who produced mirror image digit duplications in chicks by grafting a small piece of posterior border mesoderm into an anterior position8 . This is the zone of polarizing activity (ZPA) and is regulated by the sonic hedgehog (Shh) gene, which is responsible for limb patterning on an anteroposterior axis. Ectopic expression of the zone of polarizing activity cells or the sonic hedgehog gene can therefore produce mirror image deformities. Secondary signaling molecules such as the Hox genes have been implicated in the embryogenesis of mirror image deformities. Hox genes encode positional information during embryogenesis. Hox b-8 is thought to be important in the specification of the zone of polarizing activity cell positioning, ectopic expression of which has experimentally resulted in mirror image duplication9,10. The management of the ulnar dimelia deformity involves treatment of the elbow, wrist and hand8,11. The limitation of motion in the elbow is treated by extra-periosteal resection of the proximal part of the duplicated ulna. This improves forearm rotation and elbow flexion. Severe rotational deformities may require derotational osteotomy. The wrist is usually in flexion and is treated by releasing the wrist to allow extension. This may involve Z-plasty of the palmar skin, flexor tendon lengthening, volar capsulotomy or proximal row carpectomy. Flexor tendon transfer to the dorsum and wrist flexion may be required. The hand is treated by pollicization of one of the radial digits and amputation of the adjacent redundant digits. In our patient the radial index finger was of good function, size and with adequate radial index-ulna index web space. It was therefore pollicized. The ulnar small finger was of good function and position and was therefore retained. The radial small, ring and long fingers were amputated12. The wrist was normal in this patient while the elbow will need a proximal ulna resection later. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07046f2.jpg] [js07046f3.jpg] [js07046f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}