 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
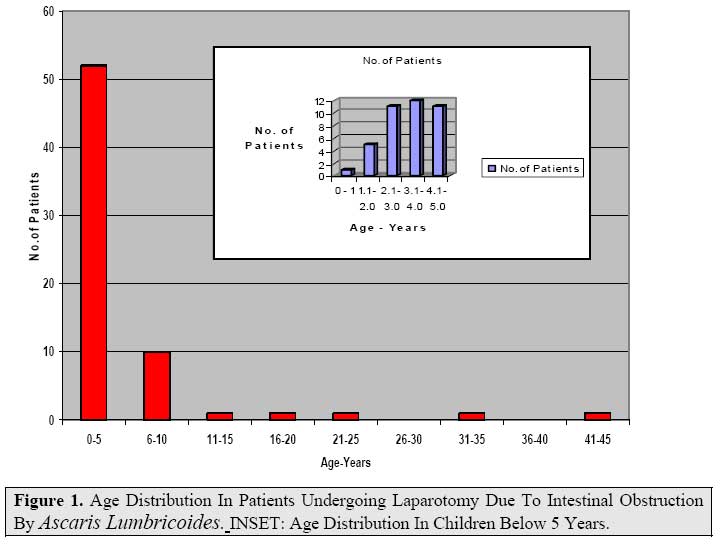
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 105-109 Laparotomy Due To Ascaris Lumbricoides at A.I.C Litein Mission Hospital – Kenya. L.D. Lugaria MBChB, MMed Surg. General Surgeon A.I.C. Litein Mission Hospital, Part time Lecturer Code Number: js07050 Background: Ascariasis is known to be a cause of intestinal obstruction particularly in children. This study was aimed at determining the burden of Ascaris lumbricoides (round worms) in as a cause of mechanical intestinal obstruction requiring laparotomy for treatment in a rural setting. Introduction Ascaris lumbricoides is a worldwide small bowel infestation with particular high prevalence in warm tropical climates, especially in low socio- economic communities with poor hygiene and inadequate sewage disposal1,2,3 . All age groups are affected but clinical manifestation and presentation vary due to the life cycle related pathogenesis3,4. Adult worms reside in the small bowel and are known to cause malnutrition, stunting and mental retardation as well as anemia1,7 . In clinical cases the worms congregate and cause bowel obstruction with or without volvulus, bowel necrosis, peritonitis and death may follow if treatment is further delayed or inappropriate5,6,8,9 . Migrating worms can cause cholecystitis, obstructive jaundice, pancreatitis and appendicitis5,8,11,12,14,15 . Adult worms migrating to respiratory tract have caused severe complications and mortality. Larval migration may cause bronchitis, asthma, pneumonia and urticaria.3,4,7 . Treatment depends on the clinical syndrome at presentation. Intestinal obstruction caused by Ascaris, whose treatment can be conservative or operative, is the subject of the current study in which laparotomy was the final definitive treatment5,9,10 . Laparotomy is done to physically remove the obstruction by either milking the worms to the colon or removing them through an enterotomy. Either procedure is performed dependent on findings at laparotomy. Patients and MethodsThis was a 5-year cross-sectional, retrospective study done at A.I.C. Litein Mission Hospital in Bureti district Rift Valley province of Kenya. The hospital is a 134 beds capacity with a catchment population of approximately 600, 000. The study population consisted of all patients whose operative diagnosis was intestinal obstruction due to Ascaris lumbricoides.. Data was obtained from the operation register, operation notes and clinical files of the patients diagnosed with ascariasis intestinal obstruction between January 2001and Dec.2005. Information on the presenting symptoms, physical findings, investigations done, findings at laparotomy, the procedure outcome and the cost of treatment were summarized on special questionnaire. The data recorded was then subjected to statistical analysis. Comparison was made with other abdominal procedures to establish the relative magnitude of the Ascaris lumbricoides as a surgical problem. ResultsOver the 5-year period, 582 abdominal operations were carried out. Sixty-nine (11.9%) laparotomies were due to Ascaris lumbricoides, being the second commonest indication for laparotomy. Ascariasis was the top cause of laparotomy in children aged 10-years and below. Out of 161 laparotomies done, 54 (33.5%) were due to Ascaris lumbricoides.. Of the 69 laparotomies, 36 patients (52%) were males and 33 (48%) females. Figure 1 shows the age distribution of patients with ascariasis. The mean age was 5 years with a range of 3 months to 44 years. The majority (79%) of the patients were aged 5 years and below; 94% were 10 years and below. The commonest symptoms were abdominal pain (81%), constipation (64%) and vomiting (58%). A history of passing worms was elicited in 35% of cases.. The symptoms duration ranged from 1 day to 7 days with an average of three days. Abdominal distension was observed in only 17% of the patients (Table 1). The commonest physical findings included abdominal mass (61%), toxic appearance (58%) and dehydration (54%).54% of the patients were under weight. Abdominal distension was observed in 40% (Table 2). The haemoglobin level ranged from 5.7g/dl to 14g/dl with an average of 10.4g/dl. peritonitis and 3 patients (6%) had gut necrosis. One patient had three worms in the appendix while one had worm impaction with small bowel volvulus. In 43 out 48 (90%), the worms were removed through an enterotomy because it was not possible to milk them distally. Worm removal with appendicectomy was done in 18 (38%) of the patients. Table 1. Presenting Symptoms in Patients Lumbricoides In 48 Patients with Intestinal Obstruction Due To Ascaris
Table 2. Physical Signs In Patients With Intestinal Obstruction Due To Ascaris Lumbricoides In 48 Patients At A.I.C. Litein Hospital (2001- 2005). *12 Of The 48 Children Were Not Weighed.
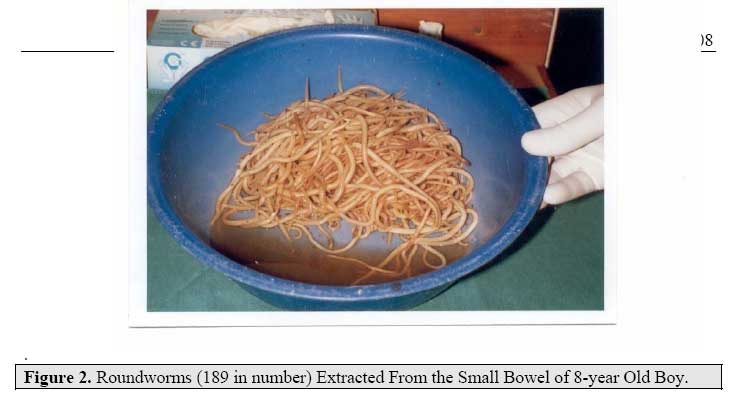
At laparotomy, 46 (96%) of the 48 patients had Ascaris lumbricoides worm impaction, 13% had peritonitis and 3 patients (6%) had gut necrosis. One patient had three worms in the appendix while one had worm impaction with small bowel volvulus. Worm removal with appendicectomy was done in 18 (38%) of the patients. In 43 out 48 (90%), the worms were removed through an enterotomy because it was not possible to milk them distally. Removal and milking of worms to caecum was performed in 3 patients (6%); while milking per se was carried out in only two patients (4%). Postoperatively, all patients survived ( nil mortality rate). The average length of hospital stay was 8 days with a range of 4-22 days. Figure 2 shows worms removed at enterotomy. The average total cost of treatment (including the surgery) was KSh.28, 916(US$ 596) with a range of KSh.20, 325(US$ 278) to KSh.50, 513(US$ 685). DiscussionAscaris lumbricoides, an intestinal nematode, is still responsible for significant surgical complications which, if not judiciously managed can be fatal1,2,3,5,8,13. Our study has confirmed what had been previously reported that intestinal obstruction due to Ascaris lumbricoides remains a childhood disease with a peak at 2-5 years5,7,8,9. Only 4 patients were aged over 10 years.. The extreme early age of three months in this study may be due to early weaning which might have exposes the baby to contaminated food. As reported elsewhere, there was no significant sex difference: 52%were males while 48% were females10,13. In our series, diagnosis was based on clinical findings. Whereas ultrasonography and plain abdominal x-rays have been shown to aid diagnosis in intestinal Ascaris lumbricoides complications, ultrasound was not carried out in these patients and the abdominal x-rays did not contribute to the making of diagnosis in these patients11,12,14. The other investigations carried out included hemoglobin level. Stool examination was also omitted (probably due to the constipation). At laparotomy 90%of cases had worm impaction without other complications. Six patients (13%) had peritonitis as well. Three patients had gut necrosis due to impaction. One patient had volvulus as a complication of the impaction while another had three worms found in the appendix. Previous studies have reported similar findings5,9,13. Where possible, the worms were milked to the large bowel. 43 patients (90%) had enterotomy and worm extraction was carried out. In 18 patients (38%), the appendix was removed as well. In three patients some worms were removed through enterotomy and others milked to the caecum. No adverse complication such as worm migration was observed in the latter5. Milking worms distally alone was carried out in only two patients. In other reports either milking or enterotomy was carried out. Appendicectomy is not a routine procedure in such laparotomies5,9. the impaction while another had three worms found in the appendix. Previous studies have reported similar findings5,9,13. Where possible, the worms were milked to the large bowel. 43 patients (90%) had enterotomy and worm extraction was carried out. In 18 patients (38%), the appendix was removed as well. In three patients some worms were removed through enterotomy and others milked to the caecum. No adverse complication such as worm migration was observed in the latter5. Milking worms distally alone was carried out in only two patients. In other reports either milking or enterotomy was carried out. Appendicectomy is not a routine procedure in such laparotomies5,9. The outcome was good with all patients surviving. The average length of hospital stay was 8 days (range of 4 - 22 days). This is attributed to aggressive resuscitation and timely intervention before serious irreversible complications set in5,9. The average total cost of treatment was Kshs. 28,916 (US$ 396) with a range of Kshs. 20,325 (US$278) to Kenya shs. 50,013 (US$685). Conclusion and RecommendationsAscaris lumbricoides infestation is still a major cause of paediatric surgical complications requiring laparotomy for treatment. High index of suspicion and timely clinical diagnosis in endemic areas are still crucial in reducing the mortality in this surgical complication where modern diagnostic aids are still unavailable or inadequate. There is need for public health activities to control nematode infestation including sanitation and waste disposal, health education and regular deworming in the under five and school going children. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07050t1.jpg] [js07050f2.jpg] [js07050t2.jpg] [js07050f1.jpg] |
| |||||||||

{kind=link}
{kind=link}