 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
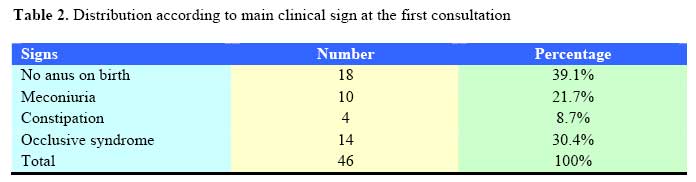
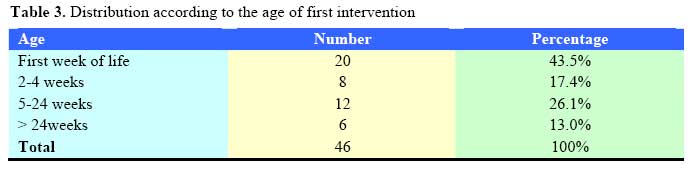
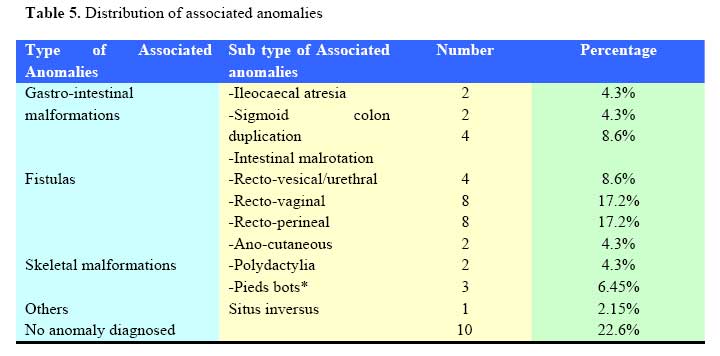
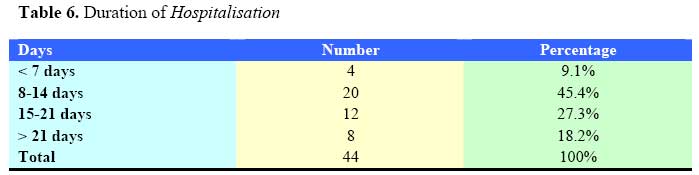
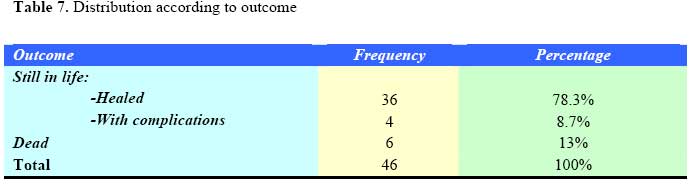
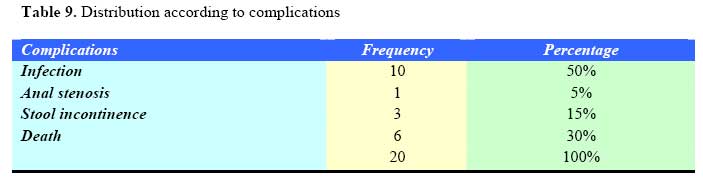
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 110-115 Anorectal malformations at University Teaching Hospital of Butare in Rwanda: A review of 46 Operative cases. M. Makanga, F. Ntirenganya, I. Kakande. Code Number: js07051 Background: Anorectal malformations (ARM) are comprised of a wide spectrum of disease that involves congenital anomalies of the anus and rectum, as well as the urinary and genital tracts. They occur in approximately 1 in 5000 live births and affect males more than females. They may present as a single or as a combination of abnormalities. Survival and prognosis of anorectal malformations depends upon the severity and number of the associated anomalies. This study was aimed at establishing the incidence, types of ARM, associated anomalies and outcome of surgery among children with anorectal malformations seen at University Teaching Hospital of Butare in Rwanda. Anorectal malformations comprise a wide spectrum of disease affecting boys and girls and can involve malformations of the distal anus and rectum, as well as the urinary and genital tracts. Malformations range from minor easily treated defects that have an excellent functional prognosis to complex defects that are difficult to manage, are often associated with other anomalies, and have a poor functional prognosis. The most common anomaly in females is a rectovestibular fistula. Perineal inspection shows a normal urethra, normal vagina, and another orifice that is the rectal fistula in the vestibule. Early diagnosis, management of associated anomalies, and efficient meticulous surgical repair provide patients the best chance for a good functional outcome. In 80-90% of newborn boys, clinical evaluation and urinalysis provide enough information for the surgeon to decide whether the baby requires a colostomy. Performing a diverting colostomy is the safest option for a surgeon without extensive experience in anorectal anomalies when faced with a baby who has clinical evidence of a rectovestibular fistula. Colostomy before the main repair avoids the complications of infection and dehiscence. Definitive repair of this anomaly in the newborn period should be reserved for surgeons who have significant experience repairing these defects. This study was aimed at establishing the incidence, types of ARM, associated anomalies and outcome of surgery among children with anorectal malformations seen at University Teaching Hospital of Butare in Rwanda. Patients and MethodsThis was a retrospective descriptive. The study population consisted of 46 children with anorectal malformations admitted to Paediatric and/or surgical Departments of Butare University Teaching Hospital and operated between 1st May 2002 and 31st May 2007 inclusive. Case records of all these cases were retrieved and analyzed for, age at the first consultation and first intervention, types of ARM, associated anomalies, and type of the first intervention and the outcome of surgery. Data was analyzed using Epidata and SPSS 11.3 computer programs. The p-value equal to 0.05 or less was considered to statistically significant. The findings are presented. ResultsDuring the study period of 5 years and 1 month, 2264 patients had operations for gastrointestinal pathology. Of these, 648 (28.6%) were children. Forty-six (7.1%) of children that is 2.0% of the 2264 of cases operated for gastrointestinal conditions, had anorectal malformations. There was a predominance of males 63% with a male to female ratio of 1.7:1. The majority (56.5%) were hospitalized in the first week of life. Six (13%) consulted for the first time at more than six months of age (Table 1). The major complaint was absence of anus in 39.1% of cases. In 30.4% of cases, the patients presented with intestinal obstruction (Tables 2). Twenty patients (43.5%) were operated during the first week of their life (Table 3). Of all these 46 neonates and children, 60.9% (28 of 46) had low anorectal malformation (LARM), 26.1% (12 of 46) had intermediate anorectal malformation (IARM) and 13% (6 of 46) had low anorectal malformation (LARM) (Table 4). Associated anomalies were seen in 77.4% of patients. The major associated anomalies consisted of fistulas (47.3%), gastrointestinal malformations (17.2%), skeletal malformations (10.75%), and cardiac anomalies (2.15%). In 10 (22.6%) of cases, there were no associated anomalies (Table 5). The majority (72.7%) of our patients were postoperatively hospitalised between 8 and 21 days with a minimum of 0 day (direct post operative death) and 42 days. The mean was 22 days (Table 6). The overall survival rate was 87%. It was 92.8% for LARM, 100% for IARM and 33.3% for HARM with a statistically significant difference (p=0.011). Thirty six (78.3%) recovered without any complications. Postoperative complications were recorded in 14 cases. Infection has been the immediate complications in 10 cases, stool incontinence in 2 cases, while anal stenosis was reported later in 2 cases. There were 6 deaths giving a 13.0% mortality rate. Two children who underwent anoplasty died due to anaesthetic complications (Table 7). According to the type of first intervention, the survival rate was 91.3%, 0%, 90.5% among those who underwent colostomy, ileostomy, anoplasty as first intervention respectively, with a significant difference (p=0.033). (Table 9) Discussion Anorectal malformations comprise a wide spectrum of disease affecting boys and girls and can involve malformations of the distal anus and rectum, as well as the urinary and genital tracts1,14. They occur in approximately 1 in 5000 live births3,4. It is somewhat more common in boys than girls and may include a single abnormality or a combination of abnormalities4,7,13. Associated congenital anomalies in neonates with anorectal malformation assume significance, as survival and prognosis depend upon the number and severity of the associated anomalies13. Some anomalies like those of the vertebra, though not letndhal, may have a direct bearing on the ultimate functional outcome of the case. Other anomalies involving the cardiac, gastrointestinal and genitor-urinary systems a may lead to morbidity and mortality during the initial management of neonates with ARM7,9,13. The incidence of associated anomalies with ARM range from 30 to 70% of cases according to various studies7,8,9,11,13. The incidence of associated anomalies basically depends upon the meticulousness with which they have been sought after. Malformations range from minor easily treated defects that have an excellent functional prognosis to complex defects that are difficult to manage. They are classified into 3 types: low, intermediate and high anorectal malformations2. The incidence of each type varies from study to study5,7,8,9,10,11,12,13. In our study, low ARM was the most frequent variety. As far as treatment is concerned, throughout the centuries, doctors have seen and have tried to treat babies born with imperforate anus. Very few patients are described, so most patients are assumed to have died without treatment. Paulus Aegineta in the 4th century wrote the earliest account of a survivor of surgery for imperforate anus. He suggested rupturing an obstructing membrane with the finger or point of a knife and then dilating the tract until healing was complete. This approach was used for many years3. Almost 1000 years later, in 1660, Scultet treated an infant with anal stenosis with dilatation. In 1676, Cooke used incision and dilatation and advised care of the sphincter muscles. In 1787, Bell suggested using a midline perineal incision to find the bowel. In 1783, Dubois acted on Littre's suggestion from 1710 by performing an inguinal colostomy for imperforate anus. Other surgeons followed suit, but almost all infants died, so colostomy remained unpopular and only a procedure of last resort. Formal perineal proctoplasty (ie, mobilization of the bowel through a perineal incision with suturing of it to the skin) was described by Amussat in 1835, and this technique gained rapid acceptance. Strictures were less common than was observed with earlier procedures. In addition to Amussat, Dieffenbach described anal transposition (1826); Chassaignac used a probe through a stoma to guide the perineal dissection (1856); and Leisrink (1872), McLeod (1880), and Hadra (1884) recommended opening the peritoneum if the bowel was not encountered from below2,3. Imaging to delineate the abnormality was first advocated by Wangensteen and Rice in 1930. Single-stage abdominoperineal procedures became widely used after reports by Rhoads, Pipes, Randall, Norris, Brophy, and Brayton (1948-1949). Stephens (1953) described this procedure and emphasized preservation of the puborectalis muscle. This surgery and its modifications were the standard approach until 19802. In 1980, the surgical approach to repairing anorectal malformations changed dramatically with the introduction of the posterior sagittal approach2,5. This approach allowed pediatric surgeons to view the anatomy of anorectal malformations clearly and to repair them under direct vision, with better visualization and understanding of the anatomy than previous approaches. Surgeons were able to understand the complex anatomic arrangement of the junction of rectum and genitourinary tract. This is the approach that is being used in our department of surgery and is giving good results. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07051t7.jpg] [js07051t4.jpg] [js07051t1.jpg] [js07051t9.jpg] [js07051t2.jpg] [js07051t3.jpg] [js07051t10.jpg] [js07051t5.jpg] [js07051t8.jpg] [js07051t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}