 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
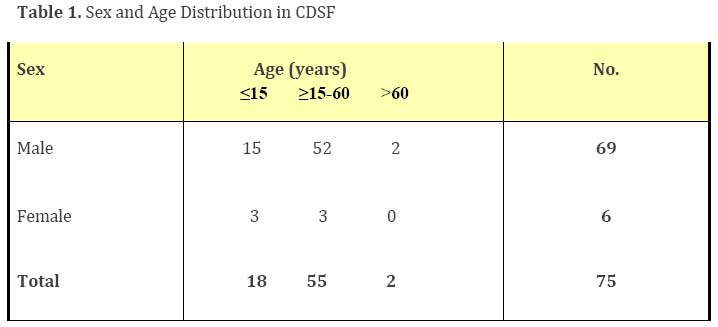
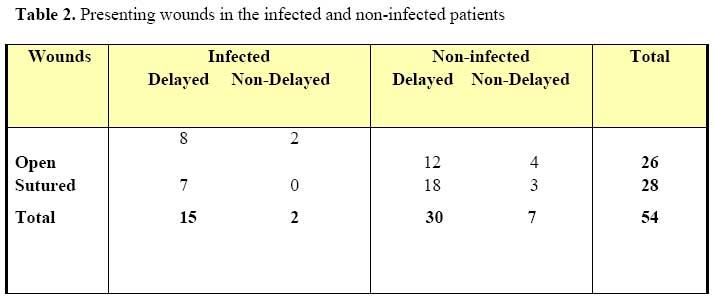
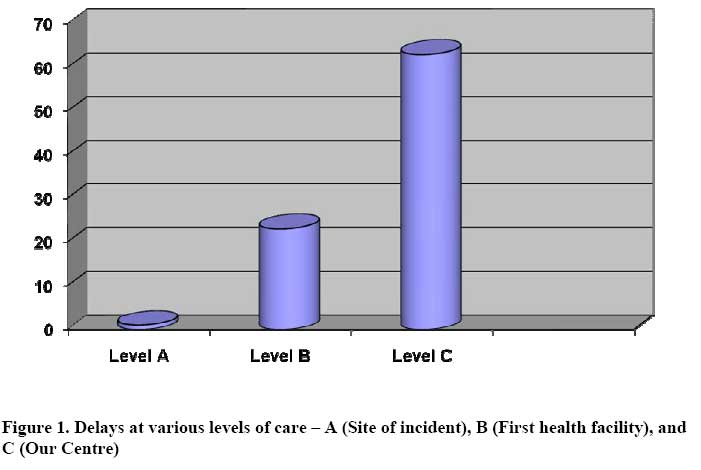
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 116-122 Causes of Delay in the Definitive Treatment of Compound Depressed Skull Fractures: A Five-Year Study from Nigeria J.K.C. Emejulu1, M.T. Shokunbi2, A.O.Malomo2, A. Adeloye2 Correspondence to: Dr Jude Kennedy C Emejulu, PMB 5025, Nnewi, Anambra State, Nigeria. Fax: +234-464-6012. E-mail: judekenny2003@yahoo.com Code Number: js07052 Background: Calvarial fractures may be linear, depressed or ping-pong, and each can be compound (open) or simple (closed). When depressed fractures become compound, they cause contamination, resulting in intracranial sepsis. All depressed fractures with scalp breach are considered compound, whether or not the breach is contiguous with the fracture. They, therefore, become almost an absolute indication for operative treatment by elevation and debridement, to avert intracranial sepsis. Definitive treatment should be within 72 hours or else it would be unsafe to preserve the bone fragments. Introduction Compound depressed skull fracture (CDSF) is a discontinuity in the skull in which one (or more) of the discontinuous edges is displaced below the inner table of the surrounding intact skull with a connection to the exterior, through the paranasal sinuses, the external auditory meatus or a scalp laceration. It constitutes about 80% of depressed skull fractures and 2.5% of head injuries, and is the most frequent reason for operative treatment in childhood head injury, in our Centre1,2,3,4 . Like all traumatic injuries especially to the head, more males than females are affected with about 70% of cases diagnosed clinically5 , requiring therefore the superior diagnostic sensitivity of computerized tomography, CT to reduce the incidence of false negatives6 . Infection, from contamination at the time of trauma, is a major determinant of long term morbidity and neglected cases are a principal cause of intracranial abscess7,8 . Dural laceration is reported to be a major predictive factor for intra-axial sepsis and focal neurological deficits9,10 . It had been established in an earlier study, that closure of the scalp alone without adequate haemostasis and debridement, does not alter the infective sequelae from CDSF11 . Elevation and debridement done within 48hours, historically, offers the best chance for an uneventful outcome, barring the severity of the parenchymal injury sustained from the trauma; recently however, a recent report advocated 72hours. A CDSF on its own, therefore, becomes a mandatory indication for operative treatment in most cases once the diagnosis is established. On rare occasions though, when the fracture directly involves a major dural venous sinus and elevation could precipitate life-threatening haemorrhage, conservative treatment has been exceptionally advocated12,13 . In our own environment, CDSF has been reported as prone to neglect, with a protracted time lag as much as three weeks between injury and definitive treatment11. This interval was reported as prolonged in patients whose wounds were sutured before definitive treatment. Why was the interval before definitive surgery longer in patients whose wounds were sutured? The previous study in our Centre had given three empirical reasons: (a) assumption that scalp wound closure was sufficient treatment; (b) expectation that scalp suturing would prevent intracranial sepsis; and (c) the fracture was simply not diagnosed. In the present study, 10 years later, we evaluated the time lag before surgery, the reasons for pre-operative delay among the patients who did not get operated within 72hours, the points in the line of management where these delays occurred, the possible reasons for the neglect of CDSF in such cases including the influence of preoperative scalp suturing on the timing of definitive treatment, and the impact of dural laceration on post-operative infection. Patients and MethodsThe 54 with complete records out of the 75cases (21 had incomplete records) treated for CDSF between November 1997 and October 2002, had their records reviewed. Essential data on each patient were collected using ward, theatre and out-patient records and subsequently, collated and analyzed. All patients aged 15years or less were categorized as children, and above 15years as adults. Operating on a patient after 72hours following trauma (the maximum historical limit of reported uneventful replacement of elevated bone fragments), was regarded as delay. ResultsOf the 75 cases, 69(92%) were males, and 6(8%) were females, a male: female ratio of 11.5:1 (Table 1). Adults were 57 (76%) and children 18 (24%). Only 2 (2.67%) of the patients were aged above 60years (Table 1). Only 54 cases had complete records. Of these, road traffic accident accounted for 27 (50%) of the cases and was the most common aetiologic factor, followed by assault 12 (22.2%), missiles 7(13%), domestic accidents 4(7.41%), industrial accident 2(3.7%), sport 1(1.85%) and fall 1(1.85%). Twenty-eight (51.9%) came with already sutured scalp wounds, and 26(48.1%) had unsutured wounds (Table 2). The affected regions of the skull were mainly frontal 30(55.6%) and parietal 16(29.6%). Dural lacerations accompanied 40(70.1%) of these fractures. Fifty cases (92.6%) were referred from other medical facilities, and 4(7.4%) presented to us straight from the site of incident. The interval between trauma and presentation to our Centre in both groups ranged 5 hours - 27days (average 4.6days), and the mean trauma – surgery interval was 12.5days. A total of 45(83.3%) cases had delayed surgery (>72hours post-trauma), 43(79.6%) of whom were referred from other facilities. There were 14 different reasons for delay, 8 of which arose in our Centre, 5 occurred at the point of first medical contact, and 1 at the site of event (Figure 1). On the whole, however, the various reasons arose 87 times among the 45 delayed cases, some patients having as much as 4 reasons for their delay. A total of 45(83.3%) cases had delayed surgery out of which 25(46.3%) presented with already sutured scalp wounds (Table 2). Cranial computerized tomography, CT was the imaging modality in 38(70.4%) cases. Seventeen patients (31.5%) had wound infections, pre-op 5, post-op 9, and combined pre-op/post-op 3; most of them (15) had delayed operations. The major complications were cranial defects 54(100%), wound sepsis 17(31.5%), post-infective hydrocephalus 1(1.85%) and stitch granuloma 1(1.85%). Most 51(94.4%), made satisfactory recovery and 3(5.6%) died in the cause of treatment. Thirty-nine (72.2%) patients were followed-up after discharge for 1 – 56months (average 8.72months). Discussion In the 5-year period (1997-2002) under review, CDSF represented 10.2% of all the indications for operations done in our service. As with most traumatic injuries, more males than females were affected, and there were three times more adults than children. A retrospective study in our Centre, 10years before, had placed the age groups as equal11. This suggests probably that even though CDSF is the most common reason for operating on children with head injury, over time, the incidence among our male adults has escalated, possibly due to a surge in traffic activities caused by the increased influx of second-hand vehicles in our country between the time of that previous report and the present study. The dominance of the frontal bone as the most commonly affected region of the skull possibly underscores the principal mechanism of injury, vehicular acceleration-deceleration, since the major aetiological factor in our study was road traffic accident. The implication of this is that road transportation represents a major factor in morbidity and mortality in our environment. Most of our patients presented on referral from other health facilities 50(92.6%), compared to those presenting directly to our Centre 4(7.4%) from the scene of the incident. This appears to be a reversal of the previous trend whereby only 39.2% of our cases came on referral from other facilities11. Proliferation of private medical facilities in our environment seems to be responsible for this current trend, and the significance lies in the need for these health care providers to be adequately and regularly informed on the diagnostic indices of CDSF and its definitive (operative) treatment modality. This could engender precise and timely referral to reduce the morbidity burden on our patients. The need for this becomes even more pressing when it is realized that of the 54 cases reviewed, 45(83.3%) had delayed definitive treatment with 43(79.6%) of them coming on referral from other facilities. Even among the 9(16.7%) that had definitive treatment at optimum time (within 72hours), 7 were still outside referrals. Being the first port-of-call for almost all our patients, these facilities and the steps taken in them become very relevant in the overall outcome from management of our CDSF cases. A little more than half of the delayed cases came with sutured wounds 25(46.3%), and a little less, 20(37.0%), came with unsutured scalp wounds, a minimal difference between the two groups in terms of delay in definitive treatment (Table 2). This, thus, challenges the previous report of pre-op scalp closure inducing delay in definitive treatment. The surfacing of CT, as the major diagnostic modality has increased the diagnostic yield in CDSF, ensuring as it were, no missed diagnosis since all the patients had correct pre-op diagnosis. We had 3 reasons for CT: (a) confirmation of the clinical diagnosis of CDSF 16(29.6%); (b) confirmation of x-ray diagnosis 13(24.1%); (c) as part of routine evaluation of head injury for other intracranial lesions 10(18.5%). For the remaining 16(29.6%) diagnosed only by x-rays, the inability to afford CT bills 10(18.5%) and faulty CT machine 6(11.1%), were the reasons. Unless otherwise indicated, CT remains the gold standard in the diagnosis and follow-up of CDSF. There were 17(31.5%) cases with infective complications, and almost all of them, 15(27.8%), had delayed operative treatment. Delay in operation, increases the chances of intracranial sepsis, and worsens prognosis, due to a secondary brain assault. Immediate elevation and debridement (with dural repair, if it is indicated) is the best treatment modality for CDSF [14]. It is noteworthy that even among the 37(68.5%) cases that did not have infective complications, 16 had unsutured, and 21 sutured wounds. It does appear, therefore, that with or without wound closure the more determinant factor in sepsis is the delay in definitive treatment. But curiously still, thirty other patients with dural lacerations and delayed treatment did not have infection. Possibly, the indiscriminate use of pre-op antibiotics or the degree of intracranial contamination may have influenced this observation. The interval between trauma and definitive operation in this study ranged from 1 to 89days, with an average of 12.5days. Though this reduced the interval almost by half when compared with a previous study (24days), it still remains a far cry from the 2 days historically recommended as the maximum post-traumatic period to allow for a replacement of the fracture fragments without discarding them, and still way behind the 72hours post-traumatic time lapse with successful replacement of bone fragments achieved recently by Wylen, Willis and Nanda7,11,14,15. No wonder, all our patients had post-op cranial defects as replacement of fracture fragments was considered a risk not worth taking at late presentation. Perhaps, the recent report by Curry and Frim16, which proved that optimizing the cerebral perfusion pressure allowed for as long as 12 days of pre-op delay under antibiotic cover without neurological sequelae, could be quite instructive. Whether this allowed for a successful replacement of fragments should be the goal of further studies. Reviewing the causes of delay in this study, we identified 3 different levels where delays occurred. Level A Site of incident to first health facility; B - First health facility to our Centre; C -Arrival at our Centre to definitive treatment. On the whole, there were 14 main causes occurring on several occasions to bring about a total of 87 reasons for delay among the 45 cases of delayed operations. Of these, 17(31.5%) had a single reason each, responsible for their delays, the other 28(51.9%) each had 2 to 4 reasons. Only 14 cases had delays at more than one level of care (Levels A and C 1; B and C 13 cases), none had delays at the 3 levels. There was a single incident of delay caused by transportation problems late at night at Level A; at Level B there were 23 incidents namely late/non-diagnosis of CDSF (15), ignorance of the correct treatment of CDSF (5), poor clinical status of patient (1), transportation difficulties (1) and attempted but failed debridement/elevation (1). At Level C, delays were in two patterns: (a) patient factors (b) hospital factors. Lack of funds reported by 21 patients, was the most common singular cause, whereas others arose from delays in the operating theatre (17), blood bank (7), radiology (7), laboratory (5), multi-disciplinary consults (5) and systemic infection (1), a total of 63 incidents. Considered separately, therefore, hospital delays (not caused by patients’ factors) arose on 42 occasions - doubling the 21 incidents of patients’ factors making the former, the most important cause of pre-op delays, by a ratio of 2:1 (Figure 1). The 17 theatre problems were issues like unavailability of personnel due to other operations taking place in the different operating suites at the same time, since in our Centre, even with dedicated suites, there are no dedicated personnel allotted specifically to the different services; lack of sterile materials and instruments due to incessant electric power failure, and even lack of water supply, on some occasions. Simply put, despite all the delays before reaching our Centre, internal hospital logistics still caused a higher number of delays; meaning that most of the efforts in trying to optimize the outcome from CDSF should be geared towards making hospital processes easier and lighter for the patients, to ensure early surgical intervention. On the long run however, 51(94.4%) patients made satisfactory clinical recovery returning to pre-morbid activities, while 3(5.6%) died in the cause of treatment. All 3 cases of mortality were males in the third and fourth decades of life, with severe head injuries (Glasgow Coma Scores of 3 - 8), and died within the first post-op week, most likely from severe primary brain assault. No patient had severe deficits or persistent vegetative state. One patient had post-infective hydrocephalus following severe intracranial sepsis, and was treated by ventriculoperitoneal shunting before discharge. Thirty-nine (72.7%) patients were followed up after discharge for 1 56 months (average 8.72 months), and only 2(3.7%) came back for cranioplasty. ConclusionCDSF, commonly an adult male traumatic injury, remains an important problem in our practice, with definitive treatment delayed in a majority of cases by avoidable logistic problems within our Centre. Pre-op scalp wound suturing did not contribute to this delay, and the late treatment inevitably leads to craniectomy and cranial defects. Dural laceration did not increase the incidence of infection. The role of peripheral health facilities, where these cases were first attended to, appeared to be significant in the morbidity burden in our environment, and continuing education programmes stressing the need for early diagnosis and referral for specialist care, with re-certification of these care givers would go a long way in checking the negative trend. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07052f1.jpg] [js07052t1.jpg] [js07052t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}