 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
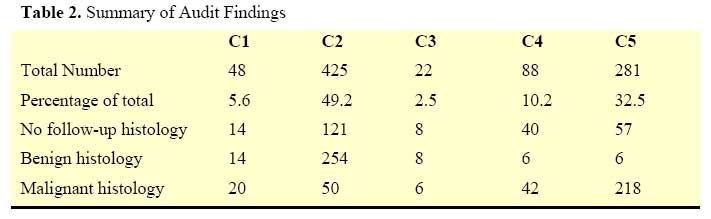
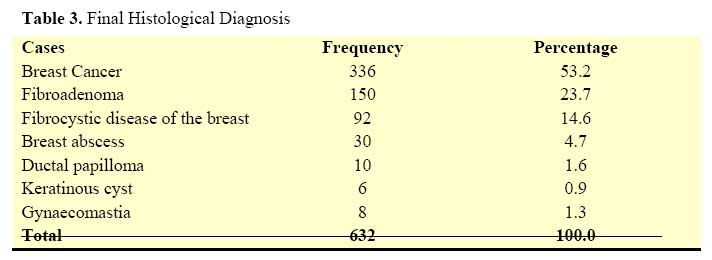
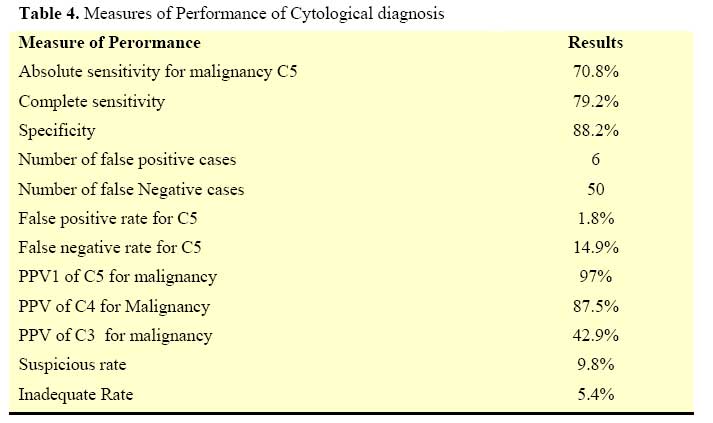
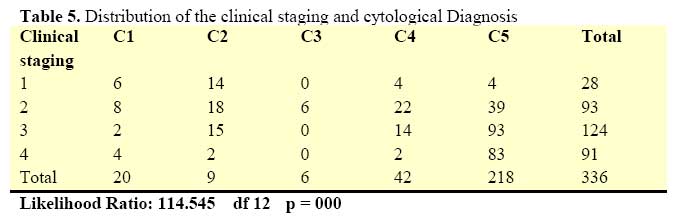
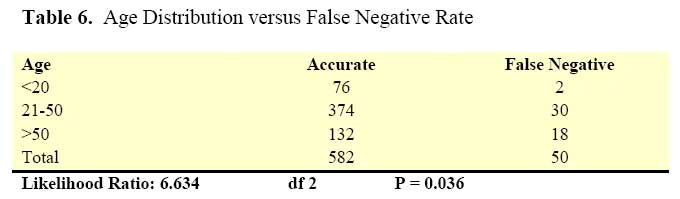
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 126-132 Breast Fine Needle Aspiration Cytology In a Nigerian Tertiary Hospital O.I. Alatise1, O.O. Lawal1, O.O. Olasode2, A.R.K. Adesunkanmi1 Code Number: js07054 Objectives: Breast disease remains a major public health issue worldwide. It is the most common cancer among Nigerian women. Fine needle aspiration cytology (FNAC) is an important preoperative assessment tool along with clinical and mammography examination in both screen detected and symptomatic breast disease. This study provide opportunity to determining the accuracy of FNAC and factors affecting false negative rate in Obafemi Awolowo University Teaching Hospital complex, Ile-Ife, Osun state Nigeria Introduction The interest in breast diseases stems from the concern aroused in patients and clinician following the diagnosis of breast cancer1 . While the overall mortality due to breast cancer has been on the decline in the developed world due to early detection and treatment2,3 , the reverse is the case in Nigeria and most of the developing countries4-7 . Indeed, breast cancer is the most common female cancer in Nigeria and patients present late with the very advanced stages of the disease8 . Fine needle aspiration cytology (FNAC) has been used as a preoperative assessment tool together with clinical and mammographic examination in both screen detected and symptomatic breast disease9 . It is relatively less invasive, rapid and cost effective in confirming a clinical or radiological suspicion of malignancy10 . It has been reported to be a very sensitive and specific test11, 12 , however, it is examiner dependent in that predictive results depend on who performs the aspiration, whether a clinician or a cytopathologist12,13 . This article is a presentation of how FNAC has been useful in diagnosing breast lumps at Obafemi Awolowo University Teaching Hospital complex [OAUTHC], Ile-Ife, Osun state, Nigeria. Patients and Methods Consecutive patients complaining of breast lumps seen between January 1997 and December 2004 at the surgical outpatient clinic of OAUTHC Ile Ife, Osun state, Nigeria and who had FNAC done were recruited for studying. They also included patients who had severe mastalgia and had FNAC under ultrasound guidance. The hospital is a tertiary referral center which serves the health needs of the semi-urban and rural communities of Osun, Ekiti, and Ondo states in southwestern Nigeria. All patients were duly informed and consented. The procedure was carried out, according to standard guidelines as described by the National Health Service (NHS) Breast Screening Programme14 , in the morbid anatomy department by resident and consultant pathologist. Following an aspirate, thin smears on three or four duly labeled slides were prepared and stained using Haematoxylin and Eosin [H &E] stains. The samples were reported based on NHS Breast Screening Programme14 protocol having the C1 defined as inadequate or unsatisfactory smear; C2-benign cells present; C3-mild atypia within some cells but probably benign; C4-suspicious of malignancy; C5-malignant cells present. Those patients suspected on clinical grounds to have mitotic lesions and those in whom cytopathology results were inconclusive also had incisional biopsies. The histopathological findings of the patients who had excisional biopsy or incisional biopsy or mastectomy were compared with their cytopathology reports. The final histological diagnosis was based on examination of the formalin fixed, paraffin embedded and Haematoxylin and Eosin stained sections of the biopsy. The definitions employed were those used by the NHS breast screening Programme and these are reproduced in Table 115, 16. Staging was done using the Manchester classification [UICC 1960]. The data was analyzed using SPSS 11.0 statistical software package. Results There were 864 patients with breast lumps who had FNAC during the study period but only 632 of them had corresponding histopathological report for comparison. Of these, 20 (3.2%) were males while 612 (96.8%) were females. Their ages ranged from 15 to 99 years with a mean age of 39.3 (Standard Deviation=16.2 and median of 36.5 years). The overall audit results are summarized in Table 2. The various final histological diagnoses are presented in Table 3. The most common histological diagnosis in this series was breast cancer in 336 (53.2%) of cases. This was followed by fibroadenoma in 150 (23.7%) and fibrocystic disease of the breast in 92 (14.5%). Using the final histological diagnoses as the standard, it would be noted that absolute sensitivity for malignancy was 70.8% (Table 4). The false negative rate for C5 (cytologically malignant smears) was 14.9%, while the false positive rate for C5 was 1.8%. The suspicious rate was 9.8% while the inadequate rate was 5.4%. Of the 48 with C4 (suspicious smears), 42(87.5%) were found to be malignant on histological examination. Among the C4 lesions confirmed to be benign on histology, there were 2 (4.2%) cases of fibrocystic disease, 4 (8.3%) cases of fibroadenoma. Similarly, of the 14 with C3 (atypia smears), 6(42.8%) were breast cancer, 6(42.8%) fibrocystic disease and 2(14.4%) fibroadenoma. Table 5 compares the cytological diagnoses of the malignant cases The implication of the high false negative rate was that a few patients that presented with early breast cancer were missed. These patients will likely present with features of advanced disease on a latter date. Most with the clinical staging (Manchester staging). As expected, it was found that the higher the staging, the higher the chances of making the cytological diagnosis of malignant condition. The age distribution of cases of false negatives was shown in (Table 6). It appeared that patients within the age 20 – 50 years with malignant lesion were more likely to be missed by cytology than other age brackets (X=6.634 df 2 P= 0.036). DiscussionIn this study, we found the absolute sensitivity for malignancy to be 70.8%, complete sensitivity of 79.2% and specificity of 88.2%. Similarly, the false negative rate for C5 was 14.9%, the false positive rate for C5 was 1.8% and the inadequate rate was 5.4%. These figures are comparable to data from some studies done in other centres11-12, 17-19. However, the false negative rate is relatively high with marginally high false positive rate patients with breast cancer in this environment present with the late stage of the disease20. Late presentation in this environment has been attributed to prolonged denial and poverty. Fear of mastectomy is another major problem deterring early presentation of women with breast cancer21,22. This, occasionally, may lead to seeking alternative modes of therapy such as herbal preparations and visiting spiritual houses in an effort to avoid the disfigurement of mastectomy. In a little way, the high false negative rate of this test may also contribute to this phenomenon. This has been related to sampling error and also the difficulty in performing required standard staining procedures such as Papanicolaou and Giemsa methods, in our laboratory. Inadequate funding of the laboratories in the country may account for the unavailability of these stains. Inappropriate staining will ultimately lead to interpretation error by the cytopathologist. Moreover, the interpretation error is found to be higher the some histological types of cancer especially lobular and tubular cancer, in patient below age 40 years, tumours of less than 2cm in diameter and early breast cancer19,23. Another reason for the high false negative rate in our study could be due to sampling error. This can be minimized by proper localization and aspiration technique23. Proper localization can be aided using ultrasound, stereotatic xray guided technique and the use of perforated or fenestrated plate24-26. Another disturbing finding in this series is the marginally high false positive rate. This portends unnecessary extensive surgery in some of our patients which is associated with physical and psychological morbidity. Sequel to the shortcoming associated with FNAC, there has been a reduction in the use of this procedure for diagnosing breast cancer in developed countries .The use of FNAC is now limited to providing accurate and rapid diagnoses for women and men with benign changes and metastatic diseases27. Core biopsy [CB] has largely superseded FNACB in most developed countries. The specificity and the sensitivity of CB are much higher with bearable false negative and false positive rates28. Several innovations have gone into the use of CB so as to make the procedure simpler and less often associated complications29. Most of the innovative biopsy forceps are not available in a developing country like ours. Moreover, histopathology results take up to seven to fourteen days before they are available. In our environment, FNACB still remains the cheapest and fastest alternatives for first line patient management. The cost of FNAC is about N750.00 [$5] as compared to N7, 000 to N10, 000[$48-$68] for surgical tissue biopsy. This should have a greater impact in developing country with limited resources and poor health care insurance coverage. Diagnostic accuracy of the report is highly dependent on the training and experience of the cytopathologist30. It is advised that caution should be employed when dealing with suspicious lesions at an early stage and in younger individuals. To improve the diagnostic accuracy of FNAC, feedback information of follow up and histology from all cases must be made available as soon as possible. Consultation between pathologists and clinicians should be facilitated and encouraged. Also, multi-disciplinary audit of difficult case should be part of the work routine. Moreover, the use of autocytofix and liquid based cytology can help to increase smear cellularity, reduce erythrocyte load and air drying artefact and eventual improvement in the diagnostic accuracy31 ConclusionIn conclusion, FNAC remains the least invasive, the most rapid and the most cost effective method to confirm clinical and radiological suspicion of malignancy, however, the test has high false negative rate. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07054t3.jpg] [js07054t2.jpg] [js07054t6.jpg] [js07054t5.jpg] [js07054t4.jpg] [js07054t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}