 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
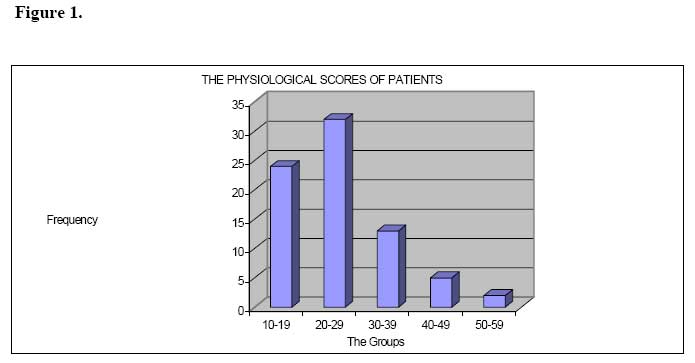
East and Central African Journal of Surgery, Vol. 12, No. 2, November/December 2006, pp. 133-142 POSSUM Scoring System In Patients Undergoing Laparotomy In Mulago Hospital. D.L Kitara, I. Kakande, B.D. Mugisa Code Number: js07055 Background: Prediction of complications is an essential part of risk management in surgery. Knowing which patient to operate and those at high risk of developing complications contributes significantly to the quality of surgical care and cost reduction in surgery. The physiological and operative severity score for the enumeration of mortality and morbidity (POSSUM) was used to score and predict the outcomes of Laparotomy in Mulago Hospital. The main objective of this study was to determine the morbidity and mortality POSSUM scores for patients who underwent Laparotomy in Mulago Hospital, between September 2003 and February 2004. Introduction Risk management is an important health care issue. Prediction of complications is an essential part of risk management in surgery. Knowing which patient is at risk of developing complications contributes to the quality of surgical care and cost reduction in surgery1 . It is therefore essential to identify and make appropriate decision on those patients who are at high risk of developing serious complications1,2 . Physiological and Operative Severity Score for the enumeration of Mortality and Morbidity (POSSUM) has been used to produce numerical estimate of expected mortality and morbidity after variety of surgical procedures.1,2 It can be used in Hospital setting to provide educational information. It integrates well in the existing hospital programs without causing any disruptions of hospital activities2. When other scoring systems were compared with POSSUM, it was shown that POSSUM results were much more useful in predicting the outcome of surgery for patients1,5 . Various studies with POSSUM in various countries with different health systems and socio-economic status to that of the UK showed that there was no change in POSSUM ability to predict outcome of surgery.1,2,5,6. In this study, a dual scoring system of POSSUM was evaluated in Mulago Hospital in Kampala. Uga Patients and Methods This was a prospective descriptive study conducted over a period of 6-months in Mulago Hospital, Kampala, Uganda. The study population consisted of 76 patients aged 13 years and above admitted for elective or emergency surgery. Day-care surgery patients and those who died immediately before surgery were excluded. The patients were assessed preoperatively and postoperatively for any postoperative complications. During the six-months, 76 patients underwent Emergency or Elective Laparotomy in the Hospital Theatres. The patients were scored with the physiological component of POSSUM just before the induction of general anesthesia. All the individual scores were computed and summed up to produce the POSSUM physiological score for each patient. The operative procedures were conducted in the same manner and using midline incision. Intraoperative blood loss, type of surgery, the presence or absence of peritoneal soiling and intra-abdominal tumors were recorded. The closure of the abdomen was done using the same suture material and equal size. The Follow-up of the patients was done up to 30th postoperative day. Patients were reviewed weekly in Surgical Out Patient Department. Telephone contacts were used, where possible. When a patient died, postmortem examinations were done by a pathologist and findings recorded. Morbidity was investigated and appropriate treatment administered to the patient as required. The risk (R1) of morbidity and mortality (R2) were calculated for each patient according to the previously validated POSSUM equations as follows: For morbidity:Log (R2 /(1-R2 ) =-5.91 + (O.16 X physiological score) +(0.19 X operative severity score). For mortality:Log (R1 /1-R1 ) = -7.04 + (0.13 X physiological Score) + (0.16 X operative severity score). Statistical data analysis was done using the SPSS version 10.0 software. A student t-test was used to compare significant differences and chi-square/Fisher’s exact test was used in testing association of categorical variables. The quality control was ensured by making the principal investigator carryout all the pre-operative and postoperative assessment, clinical examinations and measurements of parameters using standard SI units to avoid inter-observer error. Laboratory investigations were done by the same method and in standard unit. ResultsThe patients’ ages ranged from 14 to 81 with a mean of 40.4 years. M: F ratio of 2:1. Peasant farmers accounted for 52.6%, Business 27.6%, Civil servant 13.2% and Students 6.6%. Intestinal obstruction comprised 19.4%, abdominal trauma, peritonitis and abdominal malignancy 18.4% each, appendicitis 13.2% and surgical jaundice 11.8%. (78.9%) of the patients investigated had no co-morbid condition. Hypertension accounted for 11.8% and the others conditions accounted for less than 10%. A total of 55 (72.4%) of the operations were performed by the Senior Residents compared to 13 (17.1%) and 8 (10.5%) by Consultants and Senior Registrars respectively. The Senior Residents performed 86.3% of the emergency operations as compared with 9.8% by Senior Registrars and 3.9% by Consultants. For elective surgery, (44%) by Senior Residents (12%) by Senior Registrars and 44% by consultants. The Physiological ScoresThe mean physiological and operative scores were 25.22 and 21.18 respectively. The mean duration of postoperative stay was 8.46 days. Thirty two patients were discharged in the 1st post-operative week while 30 were discharged in the 2nd week. Intestinal obstruction (45.5%), peritonitis (27.3%), intra-abdominal tumor (18.2%), and surgical jaundice (9.1%) were the causes of mortality. Their average physiological and operative scores were 30.6 and 27.1 respectively. The mean postoperative day of death was 12.4. All the patients died due to septic shock. Thirty-five patients had a mortality risk greater than 50%; twenty patients had risk (21-49%), nine patients had (11-20%) and fifteen patients had (1-10%) of death. This result shows a positive correlation and a significant relationship between death and physiological score p=0.003).There is a positive correlation between death with the operative severity score p-value 0.012). The test variable (R1)
This test result shows that the formula predicted the risk of morbidity by chance because the area under the curve was just about 50%. Test result variable. R2
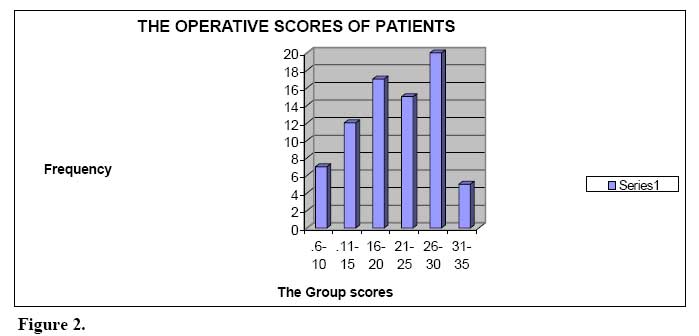
Discussion POSSUM scoring system is an effective method of assessing the risk of mortality in Mulago Hospital. The age of the patients did not significantly affect the outcome of the Laparotomy. A study in the USA indicated that increasing age was strongly associated with risk of complications but surprisingly, the risk declined for patients older than 79 years of age. The most likely explanation for the phenomenon was that there was a strong selection bias before hospitalization with older high-risk patients not being considered suitable for admission or surgery49. This observation was not made in this study probably because over 80% of the patients were below 40 years and so their age did not significantly affect the physiological score. The diagnoses did not affect the outcome (mortality), whereas Co morbidity particularly Diabetes Mellitus greatly affected the outcome (mortality) and led to elevation of the physiological score. Nature of SurgeryThe nature of surgery had a significant effect on the operative scores for the patients. On average, the emergency operations had higher operative scores (23.39). There was a positive correlation (t=4.375) and a significant relationship (p=0.000) between emergency operation and the operative scores. Similarly emergency surgery had a higher average physiological score (25.63). The risk of morbidity was significantly increased by the nature of the operation. A study involving 232,440 surgical patients at 168 hospitals in the state of Pennsylvania, USA indicated that a higher patient to nursing staff ratios is associated with higher risk-adjusted postoperative mortality rate51. This means that nursing care alone can be shown to be a robust independent predictor of postoperative deaths50,51. These results indicate that factors such as hospital resources, the availability and training of medical staffs have a significant impact on the postoperative outcome (mortality and morbidity).31,50,51. The SurgeonsThere were three categories of surgeons who were involved namely the Consultants, Registrars, and Senior Residents. The consultants operated 13 patients. All had very good physiological status. There was a negative correlation and an insignificant relationship between the 2 variables (t= 1.643 and p=0.105). Similarly their mean operative score was 17.62. For the Registrars, they operated 8 patients. There was a negative correlation (t=-0.344) between the Registrar and the operative score. The majority of the patients were operated by the senior Residents (55/76). In general, the Senior Residents operated patients with higher physiological scores. There was a positive correlation (t=2.765) and a significant (p=0.007) difference between the physiological score and the Senior Residents. Higher- risk surgery performed independently by surgeons in training was shown to be related to poor postoperative outcome. A report by UK government has drawn attention to the dangers of leaving high-risk procedures to trainee surgeons without supervision.31. In general, there was a negative correlation between the surgeons and the risks of mortality and morbidity. The Physiological Score (PS):The average physiological score observed in the study population was 25.22. This value is comparable with other studies done in the USA and UK. 31 The most frequently observed group were those between the ranges of 20-29. This score however, was found to have a positive correlation and a significant p-value with mortality (t=2.228 and p=0.029). This is consistent with the findings observed in the USA and UK31. The physiological score had a negative correlation (t= –0.019) and an insignificant and (p=0.436) with morbidity. The physiological score alone cannot be used to predict the risk of development of complications because there was other confounding factors observed28. The Operative Score (OS): The average score was 21.2. Again this average is comparable with other studies done in the UK and USA and other developing country such as Malaysia.31,38. Tribe, occupation, and diagnosis or co morbid conditions did not significantly affect the operative score. There is a positive correlation and a significant p-value for the relationship with mortality and morbidity (t=3.280 and a p=0.00) and (t=0.197and p=0.044). This observation is consistent with the findings in USA, UK31 and Malaysia.38 Physiological Score
Operative Severity Score.
Postoperative Hospital Stays (Days): The mean postoperative hospital stay was 8.46. This value was comparable with the findings in UK, USA31 and Malaysia38. Olaro (1999) observed the postoperative hospital stay of 10 days.40 The postoperative hospital stay had a negative correlation (t= – 2.894) to mortality (p=0.005). Furthermore, the postoperative hospital stay had a positive correlation (t=3.571) and (p=0.001) with morbidity. The Observed MortalityEleven out of the seventy-six patients studied died. This gave a mortality rate of 14.5%.This mortality rate was comparable with other previous studies done here in Mulago Hospital. By Birabwa-Male(1989) of 21.7% and Fiedler et al 1986 in USA (17%), Mugisa (1988) and Kazibwe (1987) (10-20%).30,42 The Laparotomy related to intestinal obstruction was the commonest cause of death (45.4%). Similar findings observed by Olaro(1999) with large gut surgery being commonest cause of mortality 28%40. Peritonitis was second (27.3%); surgical jaundice was third (9.1%) and carcinoma of the pancreas fourth (9.1%). All the emergency patients who died had very high physiological scores (>25). All the elective patients who died had high operative scores (>22). Diabetes Mellitus increases the risk of mortality. The Observed MorbidityComplications were developed in 34 (52.3%) of the 65 of the patients who survived. The factors responsible were: operative scores (t= 0.193 and p= 0.044), surgical jaundice (t= 0.202 and p= 0.040), and Peptic Ulcer Disease (t= 0.308 and p= 0.003). The operative score directly affected both the risks of mortality and morbidity31. Surgical jaundice contributed to the development of complications (t= 2.654and p= 0.010). Those patients with the peptic ulcer diseases had higher physiological and operative scores. The Predicted MortalityThe ROC curve showed area under the curve of 81.7% and the 95% c.i (71.1% to 92.4%). The Hosmer and Lemeshow test showed that the mortality formula could with accuracy predict survival 100% but only predicts death correctly in 18.2%. The Predicted MorbidityThe ROC CURVE showed the area under the curve of 58.8% and the 95% c.i (44.972.7%). The Hosmer and Lemeshow test showed that the morbidity formula correctly predicted 100% those who did not develop complications. The formula failed completely (0%) to predict any of the complications observed. The Postoperative ComplicationsRespiratory tract infection was the commonest complication (28.2%). This occurred mainly on 2nd and 5th postoperative day. Those in second day were either due to aspiration pneumonia or hypostatic pneumonia due to poor ventilation. All those who developed RTI had postoperative pain for most times. The pain therefore explains the cause of the poor ventilation and subsequent postoperative retention of secretions and development of respiratory tract infection. Andrew43 in his research found that respiratory complications were common among those who had higher abdominal incision due to atalectasis. He reported that, the main pathological changes observed were alveolar collapse of the lungs and this was observed in association with restriction of ventilation especially those patients who had a very poor pain control. Wound hemorrhage (18.2%) was the 2nd commonest. Mugisa (1988) observed a rate of (10%) and mainly among patients operated by the Senior Residents (SHO)30. He attributed this finding to emergency patients being operated in a state of shock. They were usually inadequately resuscitated and therefore the failure to localize the abdominal bleeders30. Anemia (15.5%) was 3rd commonest. This mainly occurred in patients who had blunt abdominal trauma with ruptured intraabdominal viscera. They were in most cases, found to have lost more than 1 liter of blood in the peritoneal cavity. Mugisa (1988) observe a rate of 11.3%. Wound dehiscence (4.2%) and sepsis (9.9%) were commonly seen in with peritonitis between 4th -7th postoperative day. Mugisa (1988) observed a higher rate of 15% for wound dehiscence.30He attributed this to poor surgical technique among the surgeons. Rousellot found that in USA, the incidence of wound infection was 15% and was the commonest complications experienced. This occurred between 4th –7th postoperative day with a spiking fever.45 Thromboembolism was observed in 1.4% of the cases and this was in a sickler. Stormo Aagard46 observed 15% prevalence of Thromboembolism in those above 50-years . This prevalence was higher compared to what was observed in this study population probably because the majority of the patients were younger and there were few cancer surgeries (a Thromboembolism promotion factor). Conclusionsa) The physiological severity score is predictive of outcome death but not complications. b) The operative severity score is predictive of both outcomes i.e. death and complications. c) Co morbidity: Diabetes Mellitus significantly affected the outcome of surgery (death). Recommendations1. The POSSUM score can be used in the Department of surgery, Mulago hospital for prediction of outcome of surgery. 2. The physiological score can be used for predicting mortality but not morbidity. 3. The operative score can be used in predicting both the risks of mortality and morbidity. 4. POSSUM can be used as an auditing tool in the Department of surgery and any other institution that practices surgery. 5. POSSUM can be used as guide for the referral of patients from one unit to the other thereby strengthening the referral systems among hospitals. [ Fig. 1 ] [ Fig. 2 ] [ Fig. 3 ] References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07055t4.jpg] [js07055f1.jpg] [js07055t3.jpg] [js07055t1.jpg] [js07055f2.jpg] [js07055t2.jpg] [js07055f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}