 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 27-33 Work-Related Operating Theatre Accidents Among Surgical Residents in Addis Ababa, Ethiopia. Abebe Bekele1, Berhanu Kotisso, Solomon Shiferaw2 1Assistant
Professor of Surgery, 2Assistant Professor of Public Health,
Faculty of Medicine, Addis Ababa University. Code Number: js08005 Background:With the Human Immunodeficiency virus (HIV) epidemic and infections with
hepatitis B, C and D, occupational exposures to these infections is a cause of
concern to all health care workers, especially those working in the operating
theatre in low income
countries. Introduction With the Human Immunodeficiency virus (HIV) epidemic and infections with hepatitis B, C and D, occupational exposures to HIV infection is a cause of concern to all health care workers (HCWs), especially for those working in the operating theatre1. Among the HCWs, resident doctors under-training have the highest incidence of occupational exposure as compared to nurses, interns, technicians and house keeping staff1,2. Among the residents, it has been reported that surgery residents have a six-fold higher incidence of occupational exposure as compared to other residents1,2,3. By virtue of the nature of their daily activity, surgeons in traininghave the greatest risk of exposure to blood-borne pathogens,given their numerous encounters involving the use of sharp instrumentson patients and the increased propensity for injury while learningnew technical skill sets3,4. In surgery residents, the type of exposure is mainly due to needle stick injuries and cuts, during operative procedures1,2. An estimated 600,000 to 800,000 needlestick and other percutaneousinjuries are reported annually among U.S. health care workers5. The reporting of such injuries is a critical stepin initiating early prophylaxis or treatment. Timely reporting of occupational exposures to an employee healthservice is required to ensure appropriate counselling, facilitateprophylaxis or early treatment5,6. There are limited reports from Ethiopia or the study area in relation to the rates of occupational exposure among HCWs. Information is critically lacking, especially among surgeons and surgical residents and the operating theatre staff in reference to work-related accidents and the events surrounding these accidents. Therefore, this study was conducted to investigate theprevalence and context of all work-related accidents that result in contamination with blood and blood products, including needlestick injuries, sharp object cut injuries and exposure to blood to unprotected skin and splash of blood to the face and eyes in the operating theatre among surgical residents at the Black lion teaching specialized referral hospital. It is believed that the results of this survey can serve as base-line information for further studies of similar nature, for formulations of preventive guidelines and setting up of a well-organized employee health unit in the hospital. Methods The study was a cross sectional survey. All surgical residents in training at the residency programsin General Surgery at the Addis Ababa University, Faculty of Medicine, Department of Surgery were the study population. The study hospital is the Black Lion hospital specialized referral and teaching university hospital. The hospital has more than 350 beds dedicated for adult surgical cases. The hospital has set up its first occupational health unit since 6 months before the study time that primarily deals with occupational exposure to blood and the dispensing of prophylactic drugs against HIV. During the time of the survey, there were 40 residents in training at the department. Since four residents were on vacation during the period of data collection and couldn’t be reached, the remaining thirty-six residentsparticipated in the study. Data were collected using a structured questionnaire that included survey questions about the postgraduate year of residency,the sex of the respondent, the number of past needlestick injuries, cut by sharp instruments, contact with blood to the unprotected skin and splash to the face and eyes that occurred during their residency training programme and that occurred in the operating theatre. It asked how many of the above accidents involved a high risk case. Respondents were also asked recent injuries involving a high risk patient. For the purpose of the study, a high-risk patient was defined as a confirmed or suspected case of HIV infection. The questions aboutthe most recent needlestick injury included whether it involveda high-risk patient, the perceived causes and circumstancesof injury, whether it was reported, reasons for not reportingit if applicable, and whether anyone else knew of the injury. Data entry, cleaning and analyses was performed by a statistical software EP-INFO-VER-2002. Results A total of 36 respondents completed and returned the survey forms, making the response rate 90%. As shown in Table 1, 32 (88.9%) were males, 17 (47.2%) were senior surgical residents in their 3rd and final year (4th year) of training, 13 (36.1%) were 1st year, while 6 (16.7%) were 2nd year. Of the 36 respondents, 28(77.8%) had sustained a needlestick injury inside the operating theatre at least twice during their residency (Range=2-10 times). For 13(36.1%), the accidents involved a high risk patient at least once. Cut with a sharp object, contact of blood to an unprotected skin and splash of blood to the eyes and face were reported by 11(30.6%), 27(75%) and 27(75%) of the respondents respectively. The likelihood of having needle stick injuries, blood contact to unprotected skin and splash to the face and eyes increasedas the number of postgraduate years of training increased. Table 1. Profile of Surgical Residents in Black Lion Hospital, Addis Ababa, Ethiopia - 2007.
Table 2. Characteristics of the Most Recent Injuries among Surgical Residents, Addis Ababa, Ethiopia: 2007.
Table 3. Perceived reasons for not reporting the most recent occupational injury among surgical residents, Addis Ababa, Ethiopia, 2007.
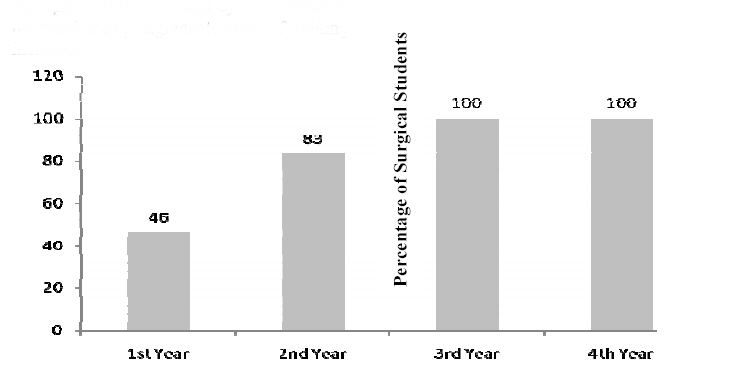
By final year of training, 100% had had a needle stick injury and contact to unprotected skin and 75% had splash to their face or eyes while needle stick injury, contact to the unprotected skin and splash to face was reported by 46.1%, 53.8% and 69.2% of the 1st year residents (Figure 1). Likelihood of Having A Needle-Stick Injury as The Years of Training Increases Among Surgical Residents at the Black Lion Hospital, Addis Ababa, Ethiopia, 2007. Similarly, thepercentage of residents who had a needle stick injury involvinga high-risk patient increased according to the year of training where 62.5% of all the final year residents reported having sustained high risk accident in the 3 months preceding the survey as compared to 7.6% of the 1st year residents. Twenty-three (63.9%) of the all study participants knew about a colleague resident who had sustained work-related accident. Information concerning the most recent occupational injury inside the operating theatre revealed that 31(86.1%) of the residents sustained work-related accident in the 6 months preceding the survey, 8(25.8%) of which involved a high risk patient. Of these injuries, 27(89.8%) of the respondents reported that the injury was self-inflicted, 26(83.8%) by a solid needle and 26(83.8%) during suturing (Table 2). The residents were 1st assistants when they sustained the injury during 13(41.9%) of the surgeries and they were the operating surgeons in 11(35.4%) of the cases. Twenty-four (77.4%) of the respondents identified a single cause for the injury, while 7(22.6%) cited two or more additional reasons. Lack of proper operating material and afeeling of being "rushed" was identified by 14 (45.1%) and 12 (38.7%) of the respondentsas major causes of the injury. Twenty-eight (90.3%) believedthat the injury was preventable. (Table 2) All of the 8(100%) of the recent high risk injuries and 22(95.6%) of the non-high risk injuries were not reportedtothe hospital’s employee health service. The most frequently cited reasons for not reporting include; “The occupational health service doesn’t exist or I don’t know if it exists in the hospital for 15(50%) of the non–reporters, it takes a long time for 6(20%), and negligence for 3 (10%). (Table 3). Of the most recent needlestick injuriesthat were not reported, 26(83.8%) were known to others: a colleague resident was aware in 20(76.9%) of these events whereas a spouseor "significant other" was aware in none of the cases. When asked whether they will report if they sustain injury in the future, 25(69.4%) of all the participants said yes. Discussion The present study revealed that work-related accidents during surgery constitute a substantial problem particularly amongsurgical trainees in a teaching hospital setting. This fact is evidenced by the fact that almost all surgical residents had sustained one form of injury in the operation theatre by their final year of training. Furthermore, nearly two-third (62.5%) of all the final year residents sustained high accident in the 3 months preceding the survey. A similar survey from Nigeria reported that almost half (53%) of surgeons sustained a needlestick injury within 3 months preceding the study7. A study done elsewhere involving550 medical students and residents during the 1989–1990training year has reported a high prevalence of needlestickinjuries (71%), and a higher frequency of injury (by a factorof 6) among surgical residents than among medical residents3,8.In our study, we have also observed that needlestickinjuries are the commonest type of work-related accidents to occur in surgical trainees. A majority of the injuries were self-inflicted and occurred during suturing. A similar conclusion was reached by other authors1,3,9. This can be explained by the fact that by virtue of the nature of their daily activity, surgeons in traininghave the greatest risk of exposure to blood-borne pathogens,given their numerous encounters involving the use of sharp instrumentson patients and the increased propensity for injury while learningnew technical skill sets 3,4. The workload imposed on surgeons on training is also tremendous. It is worthwhile to note that all recent high risk injuries and the overwhelming majority of the non-high risk injuries (95.6%) were not reportedtothe hospital’s employee health service. The tendency to under or non-report was present among various health professional groups, with the rates of under reporting being 30-60% for nurses 92% for laboratory personnel and 70-95% for physicians3,10,11,12,13. The underreporting or non-reporting of occupational accidents mayresult in a substantial underestimation of the magnitude ofthe problem. Exposure to HIV, HBV, and HCV infections has implicationsfor personal relationships, future employment, and psychosocial well-being of the injured party. It also enables timely counselling regarding the risk of exposure and preventionof secondary transmission. It also allows medical evaluation, including testing and, ifwarranted, antiretroviral prophylaxis and therapy or administration of the HBVvaccine containing hepatitis B immune globulin. Antiretroviraltherapy administered within 24 to 36 hours after exposure hasbeen associated with an 81% reduction in HIV infection14,15. There are no logical arguments to support this behavior among surgeons. However, it is believed that part of the surgical culture has been maintaining the patient first at all cost, and when an accident occurs in the operating room, the surgeon's first inclination is to continue with the operation. Surgeons might be reluctant to report accidents for fear of being barred from further practices12. Some authors have stated that one of the serious barriers to reporting include the time required to provide a medical history and blood sample to the employee health, to obtain informed consent from the patient and order the necessary tests, and to return for the recommended follow up visits. With an average of exposure of over six needle stick injuries a year for the typical surgeon, and skin contamination by blood in nearly 50% of surgical procedures, busy surgeons do not take the time to comply9. After such repeated events of injury, it is possible that surgeons may become desensitized. Personal experiences with many surgeons (Verbal communication) have also shown that a significant number of surgeons and residents do not want to use prophylactic drugs against HIV when exposed to high risk blood because of its disturbing side effects. In this survey, we have found out that a significant number of the respondents are not aware of the presence of the hospitals occupational health unit where employees are supposed to report such accidents and receive the appropriate care despite its establishment 6 months prior to the conduct of the study. The lack of information about such an important matter is something that should be critically looked at by the hospital and particularly the surgical department. Every possible effort has to be done to popularize the unit and institute a standard and regular reporting protocol. There is also a need to have working guidelines and policies that require employees to report any work-related injury timely. Bringing the occupational health unit to the operating theatres where they are easily accessible to all the operating theatre personnel might be one way of dealing with this problem. Lack of appropriate operating equipments is mentioned by some of the residents as contributory causes of injuries. In a developing country like Ethiopia where the health service is under intense economic constraint, the operating theatre is expected to be understaffed and under-equipped. These calls for a concerted effort from all major stakeholders including Ministry of Health and the hospital administration to improve to the working conditions of the operation theatre staff. In conclusion, the evidence from this survey suggests that surgical residents are being trained in a setting where the risk of work-related injuries during surgery is unjustifiably high. Compounding the problem is the huge proportion of work-related accidents which are not reported to the employee health service unit. Overall, the research indicates the need for more targeted educational and preventive measures in the hospital as a matter of urgency. While the study provides important base-line information concerning this important issue, it suffers from a small sample size, hence making calculations of some statistical tests difficult. Acknowledgment We would like to thank all the respondents in the study for their kind participation. Our appreciation also goes to the department of surgery for allowing us to do the survey and to Prof. O. Johnson for reviewing the final manuscript. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08005f1.jpg] |
| |||||||||

{kind=link}