 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
A Fourteen-Year Review of Breast Pathology at a rural referral center in western Kenya. D.M. Alterman1, R.K. Parker2, R.E. White3 1University of Tennessee Graduate School of Medicine, Dept of
Surgery, Knoxville TN, 2Indiana University School of Medicine, 3Tenwek
Hospital, Dept of Surgery, Bomet, Kenya Presented at Association of Surgeons of East Africa Conference in Mombasa, Kenya- Dec 6, 2007. Code Number: js08008 Background: Breast cancer has a low incidence in Africa compared with other
continents. Of breast cancer reported in Africa, middle and eastern
Africa is reported with the lowest incidence. In general, there is a
paucity of information about breast cancer in Africa. Breast cancer
evaluation and treatment is plagued with inadequate resource and screening
facility throughout sub-Saharan Africa. Therefore, it is difficult to
adequately assess incidence or prevalence without appropriate cancer or death
registries. To our knowledge, no data exists for breast cancer treated in
rural
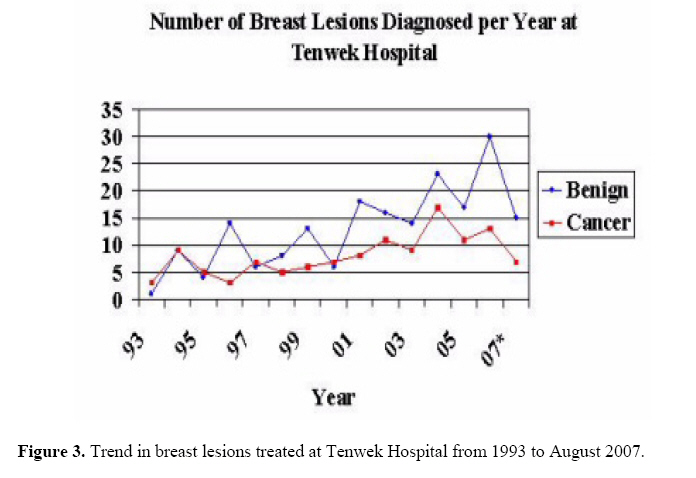
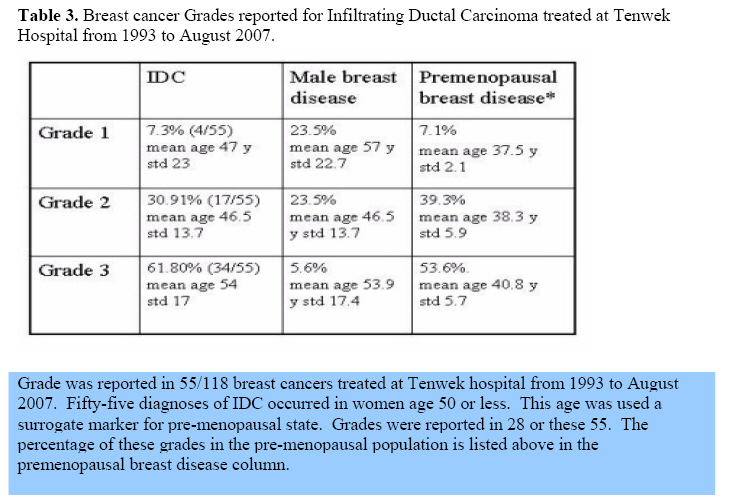
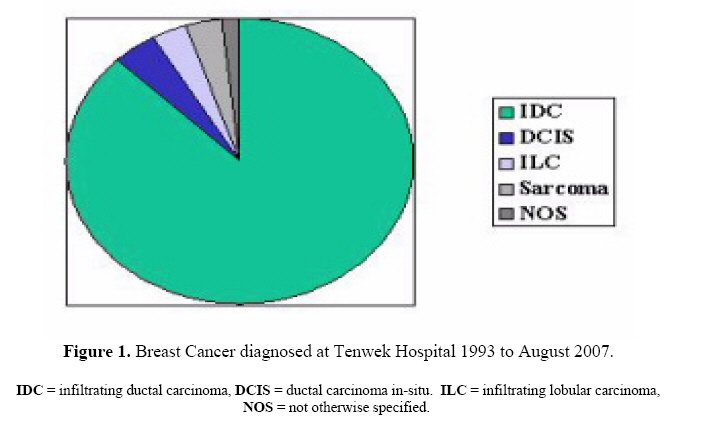
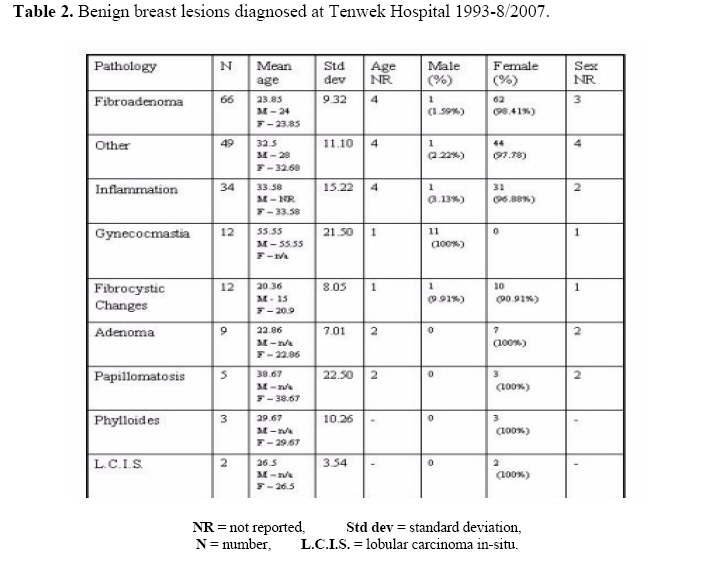
Kenya. Introduction Breast cancer has a low incidence in Africa compared with other continents. Of breast cancer reported in Africa, middle and eastern Africa is reported with the lowest incidence. Paradoxically, the ratio of mortality to incidence is among the highest in the world1. Some areas of Africa have seen an increase in incidence in recent years possibly being related to increased screening and awareness2. Typical patterns of breast cancer in Africa include a low incidence, high mortality, presentation at advanced stage and limited access to health care3. Social barriers exist such as social taboo and stigma of the disease. Data from North America shows a difference in breast cancer epidemiology, survival and histology between those of European and African descent4. These differences are also similar to the differences described above comparing what is known of breast disease in Africa and other continents. In general, there is a paucity of information about breast cancer in Africa. Breast cancer evaluation and treatment is plagued with inadequate resource and screening facility throughout sub-Saharan Africa. Therefore, it is difficult to adequately assess incidence or prevalence without appropriate cancer or death registries. To our knowledge, no data exists for breast cancer treated in rural Kenya. Several series describing breast cancer treated in Nairobi have been reported as well as a recent cancer registry based in Nairobi5-9. A small series has been reporting from neighboring Tanzania12. Little is known of the natural history, demographics, incidence and variations of breast cancer in rural Kenya. We examined breast disease treated at a rural hospital in western Kenya. Knowledge of breast cancer in this area should provide insight into disease pattern and guidance for public health efforts to focus screening, public awareness and treatment centers where they are needed most. An increased understanding of breast disease in Africa is needed to contribute to the growing literature describing different tumor biology among those of African descent.Patients and Methods Review of all surgical pathology reports was performed from January 31, 1993 to August 31, 2007 at Tenwek Hospital, a 300 bed referral center located in Bomet, Kenya. Records were searched for any breast specimen or specimen related to breast disease such as metastatic breast disease. Data is reported in descriptive terms and is limited solely to pathology records. Review of patient medical records is limited due to a number of outpatient records being discarded after a patient dies. Risk factors, clinical and pathologic stage, survival outcome, and co-morbidities were often not able to be determined. Data for hormone receptor status was also unavailable because this service is not available at our institution. It is possible that some of these patients were referred to Nairobi Hospital for this analysis, but this information is not available. Analysis and comparison of means between sub-groups was determined with Student’s T-test and variance analyzed with Fischer exact test. A value of p<0.05 was interpreted as significant. Results For the studied period, a total of 118 breast cancers were identified by review of pathology report records. Of these 118, age was reported in 100 with a mean age of 52.9 years and standard deviation (std) 16.04. Men comprised 11.02% of all breast cancers (n=13) with an average age of 69 years (std 10.6). The average age of women (n=105) was 51.2 years (std 15.6). Age was not recorded in 15 cases. The difference between the mean ages among men and women was statistically significant (p=0.000195). During this period, an increased patient volume at the hospital as well as expansion of facilities were associated with more breast lesions being treated (Figure 3). Grades were listed for 55 of 118 specimens (Table 3). Three other grades were reported with a high grade sarcoma, high grade DCIS and one grade undetermined. Of the 55, Grade 1 was 7.3% (4/55), Grade 2 was 30.9% (17/55), and Grade 3 was 61.8% (34/55). Grade 1 was 25% male with mean age of 57 years (std 22.7). Grade 2 was 23.5% male with mean age of 46.5 years (std 13.7) with age not reported in 2 cases. Grade 3 was 5.6% male with mean age of 53.9 years (std 17.4) with ages not reported in 6 cases. Age 50 years or less was specified as a surrogate marker for pre-menopausal state. All women aged 50 years or less were analyzed. This age group comprised 55 of 100 ages reported. Of the 100 ages reported, 10 in this group were men and one of these men was 50 years of age. Thus, women, aged 50 years or less, comprised 59.3% (54/91) of all women with reported ages. Of breast cancers in those aged 50 or less, 98.2% were women with a mean age of 40.3 years (std 6.6) and 50/55 were IDC. The other cancers were infiltrating lobular cancer (n=3) and sarcoma (n=2). Grades were reported for 28 of these 55 IDC. Grade 1 occurred in 7.1%, Grade 2 in 39.3%, and Grade 3 in 53.6%. Average age for Grade 1 histology is 37.5 years (std 2.1), Grade 2 average was 38.3 years (std 5.9) and Grade 3 average age was 40.8 years (std 5.7). Male breast cancer comprised 11.02% with a mean age of 68.5 years (std=10.6). The majority had IDC (12/13) with one case of NHL and melanoma of the breast. Grades were reported in 8 cases with Grade 1, Grade 2, and Grade 3 having 1 (12.5%), 4 (50%) and 3 (37.5%), respectively. Histology types were classified and are listed in Table 1. IDC comprised 89.8% (n=106), ILC 3.4% (n=4), Sarcoma 3.4% (n=4), DCIS 1.7% (n=2) and not otherwise specified (NOS) 1.7% (n=2). Of IDC histology, average age was 53.1 years (std 15.9) with men being 11.4%. Two subtypes occurred of IDC with medullary being 5.6% (n=6) and tubular being 1.9%. Medullary subtype had average age of 53 years (std 15.6). Tubular subtype had average age 52 years (std 21.2). Three cases of IDC occurred with DCIS, one with inflammatory cancer and one with paget’s disease. The three cases of DCIS are listed in Table 1 with the two cases that occurred without additional findings. ILC occurred in 3.4% with average age of 47 years (std 17.4). Sarcoma occurred in 3.4% with average age of 43.7 years (std 25.6). DCIS occurred in 1.7% with average age 47.6 years (std 17). NOS occurred in 1.75 with average age 56.6 years (std 7.8) (Figure 1). Stage was poorly defined based solely on review of pathology reports. When the patients died, their records were relocated from the record room at this institution. When records were found, documentation of stage (clinical or pathologic) was inadequate. Minimum stage was determined based strictly on the pathology report. This was based on pathologic staging as per 2002 AJCC manual for staging of cancer15 For example, if the report only said IDC as the final diagnosis then this was listed as a stage I. If the report described the specimen as IDC with ulceration, then this being a T4 descriptor was listed as a minimal stage 3B. If the report stated “positive lymph nodes” this was listed as minimal stage 2A, etc. This data likely reflects the difficulty with data collection rather than the actual stage at presentation as data from Africa usually describes advanced disease at presentation (5-9). Eight reports could not be classified. Of 100 classified, 80 were Stage I, 18 were Stage IIA, 3 were Stage 3A, 3 were Stage 3B, 1 was Stage 3C, and 5 were Stage 4. Benign breast disease was also reviewed for the same 1993 to August 2007 period. A total of 190 patients were identified. Four cases had two pathological findings and thus 192 lesions are reported. The results are summarized in Table 2. Most lesions were benign and nonproliferative lesions. One hundred ninety-two benign breast lesions, in 190 patients, from Tenwek hospital during 1993 to August 2007. Four cases had two findings that were reported individually and involved fibrocystic changes or fibroadenoma in addition to the second lesion. The “other” column involves lipomas, duct ectasia, lactational changes, etc. Fibroadenoma comprised the most common lesions (n=66) with a mean age of 23.85 years (std 9.32) and 1.59% male incidence (Figure 2). No lesions were described as having atypia or having florid proliferative changes. A few proliferative lesions without atypia were noted such as papillomas and ductal hyperplasia. These lesions have been described as having a relative risk of 1.88 for future breast cancer14. Unpublished data from this same institution also provides insight into the scope of breast disease in this area. A review of all cancer pathology at Tenwek Hospital from January 1, 1989 to August 31, 2007 was conducted by Parker and colleagues. Breast cancer was the seventh most common cancer overall, fourth most common in women and twentieth most common in men for the same time period. Discussion The number of breast cancers diagnosed at our hospital in western Kenya has been on increase at Tenwek Hospital for the past fourteen years. The diagnosis of breast cancer in men occurred at an older age compared with women. The majority of breast cancer grades were high grade. This observation remains true for pre-menopausal women as well. Benign breast disease was consistent with other data published in this country. Our data suggests that breast cancer is of low occurrence in western Kenya and that it presents in a younger group of women with a biologically aggressive phenotype. Given the nature of our review relying solely on pathologic diagnosis, it is difficult to derive incidence or prevalence data of breast cancer in this region. There was also a higher than expected percentage of male breast cancer. As previously mentioned, this pattern is also seen with hereditary breast cancer. Male breast cancer in Nairobi, Kenya has previously been described occurring in 1.59-3%9,14. Similar data has been reported from elsewhere in East Africa. Amir et al12`describedfifty patients over a six-month period at a district hospital in Tanzania who were analyzed for type of breast cancer and stage. Most had advanced breast cancer, with 76% having stage IIIB and 10% stage IV. All of these patients were reported to have had IDC. Most patients were pre-menopausal, 90% being less than 50 years old. Lacking from our data is information of hormone receptor status and genetic data regarding oncogene expression and/or polymorphisms that may contribute to the disease burden in this area. It is known that mutations in BRCA occur in higher prevalence in individuals of African descent (18%) compared with those of European descent (16%) when a large cohort of high-risk individuals is screened13. In 2006, Nyagol and colleagues5 reviewed 158 women in Kenya with breast cancer to evaluate prevalence of hormone receptors and Her-2/neu expression. The trend noted with breast cancer in sub-Saharan Africa involves a younger onset compared with developed countries, a lower incidence overall, and a more advanced stage at presentation. The majority of breast cancer was grade III, as was noted in our data, and the majority presented with advanced breast cancer (Stage III or greater). Over expression of Her-2/neu was associated with high grade tumors. Hormone receptor positive status was associated with both high grade and post-menopausal status. Of note, 28% had all three negative ER, PR and Her-2/neu and 6% had all three positive. Seventeen had ER+, 35 had PR+, 32 had both ER and PR+. At least one steroid hormone receptor was present in 53%. About 50% were premenopausal. Absent the receptor status data, the other features of this study from Kenya are similar to our data and it would be interesting to know if this population treated in Nairobi reflects the population found in rural western Kenya where our data was collected. An earlier review examined breast cancers treated in Nairobi from the early 1980’s and noted a similar trend with 88% being IDC, 71% poorly differentiated and an increasing incidence from age 20 until menopause with a decline after menopause. This incidence pattern is in contrast to the rise beyond menopause noted in North America and Europe6. Benign breast disease has previously been reported as series in Kenya with 650 cases from the early 1980’s. Similar to our data, and others, fibroadenoma was the most common lesion with a peak incidence at around age 207. Many breast cancers in developing countries present with locally advanced disease. Optimally, adjuvant chemotherapy may improve the response to surgery as well as allow for conservation therapy. The response to adjuvant therapy is also an important indicator of prognosis. While multimodal therapy is recommended there are significant barriers to obtaining this in developing countries. Alternatives to anti-estrogen medical therapy should be explored such as oophorectomy 10. Lack of multi-modality therapy for patients with breast cancer is a reality for most in Kenya. A retrospective review was carried out for a recent 11 year period in 374 patients treated for breast cancer at the national referral center in Nairobi, Kenya8. During this time, only 22 received adjuvant chemotherapy, 21 had chemotherapy for palliative purposes. Adjuvant radiation therapy was received by 46 and 53 had it for palliative purposes. Hormonal therapy (tamoxifen) was given to 126 during this time. Interestingly, only one man was included in this group of 374 reviewed. This is in contrast to the 11% noted in our rural review and this differs from the recently reported Nairobi Cancer Registry listing male breast disease at 3%9. Less than 10% of patients had Stage I disease, with 60% having at least Stage III disease. Even with this large percentage of advanced breast disease, only 6% received adjuvant chemotherapy. Follow-up for this group was very limited. The reasons for this sub-optimal approach as given by the authors include prohibitive cost and physician awareness. Additional reasons cited as presenting difficulty for multimodal therapy for breast cancer in Africa include lack of advanced pathology testing (e.g. hormone receptor status)16. While tamoxifen is generally available, including at our rural hospital in western Kenya, without receptor status knowledge empiric therapy for all increases the cost burden as well as presumably raising the risk-benefit ratio with the added risk of thromboembolic events and cervical cancer. It is not known what percentage of our patients received any therapy beyond surgery. Tamoxifen is available locally but not the pathology resources to determine hormone receptor status. Support for breast cancer patients is limited in developing countries. In other regions, there may be a belief that breast cancer is the result of a curse or supernatural influence; therefore, it may only be treated with supernatural therapy16. The stigma associated with such a malady may fuel secrecy among families and reluctance to seek medical attention until it is far advanced. Lack of awareness and social taboos about the disease often impede the process of screening, treatment and support for the patient11. Increased public awareness and screening programs are indicated for those areas that breast cancer occurs at a younger age and more aggressively. An additional feature of our data is that it emphasizes the global difference in breast cancer between Africans and persons of African descent compared with other races. A significant percentage of women with breast cancer in our series were pre-menopausal and had high grade carcinoma. This issue has been documented more extensively in North America. Newman reviewed this topic and reported an earlier onset and more aggressive phenotype in African-American women compared with Caucasian-American women3. There is a lower incidence in African-American women overall, but a higher incidence for American women younger than 45 years3. African-American women are more likely to be diagnosed with node positive, high grade, hormone receptor negative breast cancer compared with Caucasian-American women. Incidence of breast cancer in North America and Europe is estimated to be approx 100 per 100,000 persons compared with the estimated lower incidence in western Africa of 20 per 100,000 3,17. Similar data has been found with comparison of women from the United States only. A lower incidence in women of African descent from SEER (Surveillance, Epidemiology and End-Results) data showing an age-adjusted breast cancer incidence of 119 per 100,000 women compared with 141 per 100,000 Caucasian-American women1. The reason for lower incidence of breast cancer in Africa is unclear and may be related to lifestyle protective factors such as reproductive patterns. It should be noted that there is paradoxically a briefly increased risk of breast cancer in the post-partum period, but the influence of this phenomenon is unclear. An interesting relationship noted by Newman involves the similarity in features between African-American and African women with breast cancer in that both groups tend to have an earlier onset, higher grade, more advanced disease at presentation and lower survival rates. 3 The reason for higher mortality from breast cancer in African-Americans is unclear but has been speculated to be related to socioeconomic status and medical co morbidities. A recent review examined this issue and when accounting for these factors, the mortality risk for African-Americans was 28% higher1. An increased understanding of breast cancer among Africans is likely to benefit both groups. A review by Chen and colleagues18, examined breast cancer histology comparing US women of African descent with non-African descendents. They found African-American women had a higher chance of having high-grade tumours, more necrosis and oestrogen receptor positive tumours. After controlling for socioeconomic status, height and weight, and use of tobacco and alcohol, reproductive history and access to health care – these differences remained18. They quote data of African-Americans having an overall lower 5-year survival from breast cancer of 62% compared with 79% with whites21. Newman et al19 reviewed the SEER database of patients seen in Detroit from 1990 to 1999 with breast cancer. African-American women were found to have larger primary tumors, more medullary cancer, more Oestrogen and Progesterone hormone receptor negative tumors, and poorer survival. Mean survival for African-Americans was 45.2 months compared with 49.9 months. The authors note that hormone receptor negative and high-grade medullary tumors are features seen with hereditary breast cancer and this was also noted in AA women in this review20. Social factors and access to medical care cannot adequately explain these differences. Data from western countries where breast cancer natural history, survival, histology and receptor status has been more extensively documented show a clear racial difference in breast cancer tumour biology. These data suggest a difference in tumour biology of patients with breast cancer of African descent. Further investigation should emphasize characterizing risk factors and epidemiologic data to better understand the breast cancer burden in East Africa. Relating this data to study of tumour biology including hormone receptor, her-2/neu status and histology should provide focus for further improvements in breast cancer treatment in Africa. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08008f2.jpg] [js08008t2.jpg] [js08008t1.jpg] [js08008f1.jpg] [js08008t3.jpg] [js08008f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}