 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 51-59 Ambiguous genitalia in rural Africa and the complexities of management: Which way forward? P.M Nthumba, L.L. Carter, Jr, , D. Poenaru Department of Surgery, AIC Kijabe Hospital, P.O. Box
20 Kijabe 00220, KENYA Code Number: js08009 Intersex disorders are amongst the most controversial conditions managed by doctors today. Although the diversity of their presentations demands broad classifications to help standardize management guidelines, each patient remains unique, requiring individualized care. The authors review the prevailing schools of thought on gender determination, assignment and re-assignment of intersex patients. The “liberal” views on sexuality, as espoused in current Western literature, vis-a-vis the “traditional” views of the average rural African community on sexuality are noted. The case histories of four patients highlight the diversity of presentations as well as the challenges in their management in a rural Kenyan hospital. ABBREVIATIONS
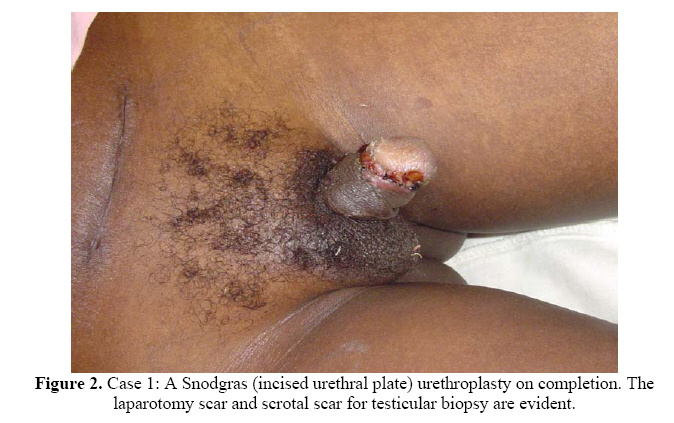
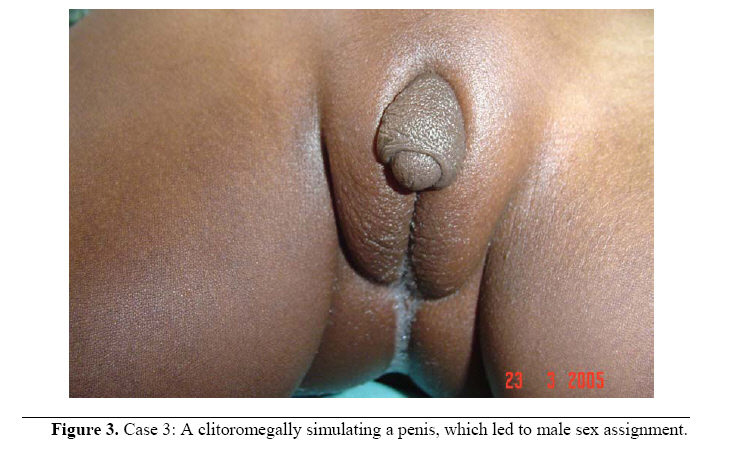
Introduction Normal sex differentiation begins with the establishment of chromosomal (genetic sex) at fertilization. Genetic sex directs gonadal differentiation (gonadal sex), which subsequently determines hormonal secretion, resulting in the development of appropriate external genitalia (phenotypic sex). Gonadal sex is determined by the presence or absence of the Y-chromosome, which, when present, has a testis-determining action on the indifferent gonad. The interruption of this normal sequence of events may lead to incomplete gonadal or genital development, resulting in discordance between genetic, gonadal and phenotypic sex: termed ambiguous genitalia, or the intersex state. Children born with intersex disorders comprise about 1.7% of all live births1.Intersex disorders are among some of the most distressing problems encountered at birth because of the uncertainty that clouds the newborn’s most basic identity2and may be the most devastating condition after perinatal mortality, to face any parent of a newborn. The birth of a child with ambiguous genitalia constitutes a social emergency; requiring rapid determination of a definitive diagnosis, to facilitate the development of a suitable treatment plan that will minimize medical, psychological, and social complications3. Human society has historically organized itself around the distinction of the sexes. Most people take it for granted that humanity comes in two mutually exclusive sexes: male and female4, 5 resulting in overt and unconscious societal pressures that bear heavily upon the intersex child and family6. In the majority of patients with intersex disorders, the appropriate sex of rearing will be obvious, and only a few patients have genitalia that are so ambiguous or inconsistent with other aspects of reproductive function that the sex of rearing becomes problematic7. When the gender of an intersex child is uncertain or was wrongly assigned at birth, subsequent gender assignment or re-assignment poses some of the most emotional and contentious ethical dilemmas encountered in any area of medical practice8.There are no solid long-term outcome studies on patients managed with intersex disorders in current literature, and discussions on this subject logically spark off strongly-held personal and cultural biases. Case Reports Case 1 KM, the first child of educated parents, was noted to have ambiguous genitalia at birth. The parents decided to bring up the child as a boy, declining any intervention at the time. Chromosomal studies performed at age 3 years were reported as 46, XX (genotypic female). At the age of 10 years, he and his parents noticed gradual enlargement of the breasts, and at age 12, brought him to hospital for surgical correction. On examination, he had a feminine body habitus, with gynecomastia; a perineal hypospadias with a severe chordee and bifid scrotum with a palpable gonad in the right hemiscrotum. There was no vagina. A pelvic ultrasound examination revealed a mass, suspected to be the uterus. He underwent bilateral subcutaneous mastectomies were performed, total abdominal hysterectomy and a left salpingo-oophorectomy. A Snodgras hypospadias repair with chordee release completed the required reconstruction. Histological examination of the ovarian tumor revealed a benign ovarian teratoma, while a testicular biopsy identified seminiferous tubules with oligospermatogenesis, establishing the diagnosis of true hermophroditism. He is currently in school, and appears very well adjusted. Case 2 A thirty-five year-old single woman presented with complaints of abnormal genitalia, a masculine voice and poor breast development. While growing up, she noticed that she was able to void while standing, her breasts failed to enlarge, and her voice deepened, unlike other girls. At age thirty-five, she was still single, a pariah status in her community, which practices polygamy. On examination, she had distinctive masculine facial features, a hooded phallus with a chordee, a perineal urethral meatus, and bifid scrotum with bilateral testes. A pelvic ultrasound exam was consistent with a normal male pelvic cavity. The diagnosis of a male phenotype with hypospadias reared as a woman was made. After counseling, a hypospadias repair, and male gender-reassignment were achieved.. The patient subsequently got lost to follow-up. Case 3 A 16 year-old boy was brought with complaints of urethral bleeding, perineal hypospadias and gynecomastia. The abnormal genitalia were noted at birth, but no treatment was sought for or offered at the time. Examination revealed a feminine body habitus with well developed breasts, a small hooded phallus with severe chordee and a perineal hypospadias. He had a bifid scrotum with no palpable gonads, but no vagina. We explained the fact that this ‘boy’ might be a ‘girl’ and needed further investigations to determine this. There was immediate disagreement in the family: the patient wanted to remain a boy, but have the tests, while the family wanted an immediate ‘sex-change’ with no further investigation. They left to confer and return later for definitive care, but have not been seen to date, more than two years later. Case 4 A 3 month-old baby with ambiguous genitalia raised as a boy was brought to our institution. Examination revealed a healthy 3 month-old girl with a clitoromegally, but otherwise normal female external genitalia. A minilaparotomy revealed a normal uterus, fallopian tubes and ovaries. The parents were informed that this was a girl, and required at most a name-change and a reduction clitoroplasty. The decision making process required the community elders input. Three weeks later, the elders consented for the surgery and gender re-assignment. Table 1. *Traditional classification of Intersex.
* This simplified table of traditional classification of intersex disorders is compounded by two further important determinants – gender of rearing, and brain sex. Correct diagnosis permits the patient to be managed appropriately as suggested in this table. Discussion The histories of these four patients illustrate the complexities involved in the management of patients with ambiguous genitalia in rural African healthcare settings. The history of successful reconstruction and integration into society, as reported in case 1, is unfortunately the exception. Patient histories similar to those of Case 4 abound. Problems face the intersex patient in our environment from all sides – from the community in which the individual is regarded with suspicion, even fear, and from the healthcare givers, because of lack of experience, misunderstanding or perhaps discomfort with the concept of intersex, a problem that appears to be universal7, 9. To overcome this, some authors have recommended that healthcare workers be given considerably more education on intersex conditions10. In Kenya, only 20% of the total deliveries occur in healthcare institutions - 80% are conducted at home by traditional birth attendants. Irrespective of the setting, the person conducting the delivery announces the gender of the child to the mother, and other relatives. The gender assigned at birth establishes the basis for the name and sex-of-rearing of the child, reinforcing its identity as a member of that community. This is normally based on the appearance of the external genitalia. The presence or absence of a penis is the paramount differentiating feature. Some communities in southern Africa use the degree of scrotal development as the main gender determinant11. If not carefully examined, features such as micropenis (likely in case 2) or clitoromegaly (cases 3 and 4) may lead to an inappropriate gender assignment, with far-reaching life-long psychosocial and psychological effects. Most African communities are bipolar, recognizing only two genders, male and female. Recent activism by certain groups in the developed world, fuelled by increasing numbers of transsexuals, has led to pressure towards the acceptance of a neutral gender – neither male nor female. These groups expect the parents of intersex children to raise them ‘ambiguously’, until the age of gender self-determination1,8,12,13. The reality however, even in these communities, is that parents plan for and expect a boy- or girl-child. The recognition of parental acceptance as a fundamental determinant of the success of any management strategy in the care of intersex children is therefore critical7. Schools of thought There are two main schools of thought in gender determination, both supported by a mixture of sparse scientific data and strong emotional or traditional cultural overtones. Central to the arguments of both is the outcome of the patient “Joan/John”, perceived to have been a successful post-genital trauma sex-reassignment by one school, but deemed a total failure by the other14,15. One school of thought, championed in the West by Money, proposes that gender is primarily the result of societal (post-natal) and psychosocial influences, as defined by the sex-of-rearing, name, mode of dressing, and assigned social roles, amongst others. It recommends a proactive approach to the management of intersex disorders, with institution of prompt decision making, encouragement of gender-specific role-playing, and early, aggressive surgical therapy, if indicated16,17,18. This teaching is consistent with evidence that a child’s sex-of-rearing firmly embeds his/her gender by the age of 2.5 years7,16,18,19, and also with established rural African practice. Defining gender-specific social roles are especially important in the rural African community, and are imprinted early through the naming process and gender role-modeling - the girl-child is ‘mommy’, while the boy-child is ‘daddy.’ Even in the absence of the biological father, a community-recognized father-figure permits appropriate role-modeling. The alternative theory proposes that gender is defined during intra-uterine life, and that the effects of intra-uterine brain androgen-imprinting overrides post-natal social influences, and may even eclipse chromosomal sex. This theory is mainly based on the experimental results of the effects of intra-uterine androgens on the sexual behavior of mice20,21. Proponents argue that there is no data providing adequate reasons for using surgery before the child has the developmental capacity to participate in decision-making10.Unfortunately, the recommendation to withhold all non-essential early genital surgery in the intersex child overlooks the fundamental role of parents in ensuring a child’s physical and emotional well-being22, and may be harmful to the child’s psychosocial development. We currently know little about the effects of hormonal imprinting on the fetal brain. It is therefore impossible to predict the full impact of corrected and uncorrected genital malformations on the life of the individual, family and social contacts. Moreover, among humans, there is no convincing evidence that variations in prenatal androgen exposure indelibly influence adult sexual orientation6,7. Indeed there is some evidence that sexual differentiation in the brain actually precedes the onset of gonadal secretions23,24. With all the medical-science made advancements to date, it is astonishing how little we know about the establishment of our most basic individual and social identities25. Management There are three domains of gender development: gender identity (developing in infancy), gender role (acquired during childhood) and sexual orientation (occurring during teenage years through adulthood)7,26. These domains form the framework within which to develop optimal management strategies for these children and their families. Irrespective of the model used, the goal must be the development of the child into a well-adjusted, psychosocially stable individual who identifies with and is happy in the chosen sex.The family and healthcare provider(s) must realize that any treatment strategy may fall short of creating an absolutely normal child, and that long-term counseling and support for the patient and family may be necessary17. Lev-Ran in 1974 described the American society as openly sex-oriented, and contrasted it to the Russian society, where, although an intersex disorder was considered abnormal this was so only within the borders of the sex assigned at birth.His patients had no doubts about the sex-of-rearing. Sex was assigned “once and for all”18 – affirming that the local culture greatly influences the criteria for gender assignment and re-assignment27. The Indian Hindu community may be the only community in the world to recognize a ‘third’ gender, the Hijaras, a community of intersex individuals that lives separately, but serves important social and religious functions28. Their existence is shrouded in religious superstition, myth and legend. They probably owe their way of life historically, to the absence of corrective surgical techniques. With the availability of corrective surgery9, it is possible that they will become extinct. In managing patients with intersex disorders care-givers must be conscious of the complexities of diagnosis, and be sensitive to the desires of the child, family, and community, as well as the presence or absence of social services11, 17. A complete diagnosis shortly after birth, allows for the most appropriate gender assignment. Unfortunately, the means to this (including chromosomal studies, enzyme and hormonal assays, and androgen receptor levels), as envisaged in most Western healthcare systems, are unavailable to care-givers in most African healthcare settings. Indeed, the only available information may be the history, physical exam, the occasional ultrasound and/or a buccal smear for Barr bodies. Socio-economic factors in these communities dictate that hospital follow-up will be irregular or totally impractical, and that the first contact between the patient and the physician may also be the last. Optimal care must, therefore, be given during this initial contact. This reality is reflected in the case studies described earlier - three patients are yet to be return, more than two years after the last contact. Protocols Gender development is the product of complex interactions of multiple factors including genetic, gonadal, external genitalia and environmental (societal) pressures, in addition to many other unknown determinants. Consequently, whereas standardized management guidelines may be desirable for intersex disorders, treatment for each patient must be individualized. Obstacles that stand in the way of standardized protocols include the lack of comprehensive outcome data; problems with poorly understood interactions among the individual, social environment and other variables affecting human sexuality, and the fact that concrete models cannot be used to predict future adult gender identity and sexual orientation during infancy7. Traditional teaching divides intersex disorders into four groups: the true hermaphrodite (TH), mixed gonadal dysgenesis (MDG), and female and male pseudohermaphrodite (Table I). Although each patient is a unique individual requiring individualized care as noted above, sufficient similarities within each group permit for broad strategies of management. Thus, most female pseudohermophrodites, for example, are virilized females, due to congenital adrenal hyperplasia (CAH) - likely in case 4. Treating and raising such children as females makes the best sense. The presence of a gonad in the scrotum implies adequate levels of intra-uterine testosterone and Müllerian Inhibiting Substance (MIS), as well as exposure of the brain to circulating androgens, and these children are best raised as males. The size of the phallus only implies availability of androgens, and does not necessarily correlate to the sex of the child. In the absence of gonads below the internal ring, the diagnosis is much more difficult, and the sex assigned may not be appropriate. Fortunately, most times, the sex assigned is appropriate7. Anecdotally, in the Western world, most babies were raised as female because the genitalia were easier to reconstruct29. Current practice bases these decisions on an amalgam of factors, including genetic sex, phenotypic sex, and the therapy thought most likely to result in sexual function and fertility (if possible)17. In the absence of sound scientific data to the contrary, this practice gives the best results, in the context, and within the constraints of management of these patients in rural Africa. There are multiple reasons for the slow and controversy-ridden evolution of sound management protocols for patients with intersex disorders. These are true in the developed world, but are even more obvious in developing countries. The care of the intersex patient is unavailable, inadequate or expensive, with multiple visits to multiple care-givers, spanning broad time-scales, and in different institutions. These visits cost money which in rural communities, is frequently from a single source, and the family has to choose between the care of the patient and the basic needs of the rest of the family. The reality that these patients require lifelong follow-up and occasionally lifelong medication, places an even bigger burden on them and their relatives, leading to poor long-term follow-up and outcomes. Furthermore, whenever possible, appropriate follow-up demands regular physical examinations that include exposure of external genitalia. While this may be acceptable for a child, it may be unthinkable to the adult. This discomfort is further heightened as the care-giver delves into the patients’ sexual activities and/or thoughts, another taboo in most African cultures. The resulting emotional and financial strain imposed on the patient and family becomes almost palpable. Unfortunately even in the developed world, where lifelong follow-up in many fields of medicine is the rule, there are no data on long-term follow-up of intersex disorders, and the conclusions of the multiple short-term follow-up studies are dogged in controversy, or even contradiction14,15. Poor dissemination of information on intersex disorders and their management amongst healthcare providers and parents and patients, has led to significant misunderstandings. A feeling of guilt and/or shame amongst parents/patients, made worse by poor understanding of intersex disorders by the community, may lead to social isolation and sexual dysphoria26. In most rural African communities, the individual is a member of the community and the ‘rights’ of the community override those of the individual - the community defines and gives identity to the individual. Thus in Case 3, where the assigned gender was found to be at variance with gonadal and genital sex on medical examination, the elders, custodians of the community, had to be approached by the parents, to consent the gender re-assignment. Additionally, in gender reassignment and surgical intervention, therapeutic goals must include an attempt to ensure that adult social function and sexual fulfillment are considered. Case 2 is an unfortunate example of a man robbed of the opportunity of living his life, because the family had no access to healthcare. Conclusion Intersex patients should be managed in the context of the community they are to be raised in – the community is their life. The time in hospital is a temporary sojourn out of that environment. Societal acceptance and integration of an individual within the rural African environment is imperative - otherwise one risks creating social outcasts, “modern-day lepers”, with a domino effect on the extended family. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08009f3.jpg] [js08009f1.jpg] [js08009f2.jpg] [js08009.zip] [js08009f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}