 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
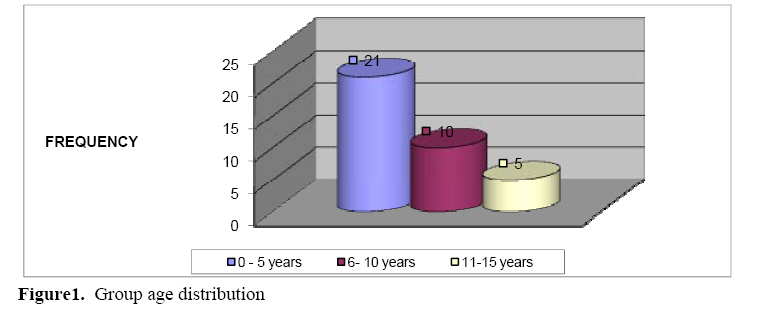
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 60-65 Paediatric Cancers at Butare University Teaching Hospital in Rwanda. M. Makanga, M.A. Ayinkamiye, L.Ngendahayo, I.Kakande Butare UniversityTeaching Hospital, NUR, Rwanda Presented at Association of Surgeons of East Africa Conference in Mombasa, Kenya- Dec 6, 2007. Code Number: js08010 Background: Cancer is an
important cause of mortality in many of the economically developed nations of
the world. More than 10% of all deaths in children below 15 years of age are
caused by malignant diseases in developed countries. In the developing world,
childhood cancers are yet to be recognized as a major pediatric illness due to
several other competing causes of death like diarrheal illness and respiratory
illness. Although, Cancer is rare in children aged less than 15 years1, it represents a main concern for parents, families, and health professionals to care for children affected with cancer. The problems confronting Paediatric oncology in Africa are many. They are linked to:
These lead to low survival and cure rates: The patients’ survival at 5 years is ≤ 50% in developing world whereas cure rates in developed countries represent 75-80 %1. In Rwanda there is no possibility of effective, efficient management of cancer after diagnosis is confirmed for lack of an established oncology Department. A review of literature shows that no specific study on cancer in children has bee reported from Rwanda. It was with such background that a study was undertaken on childhood cancers in Butare university Teaching Hospital. Results During 7 years period of our study, there were 20,171 admitted patients in the five departments of Paediatric, Surgery, ENT, Ophthalmology and Stomatology of whom 36 (0.18%)patients had childhood cancer. Table 1 shows the annual distribution of children with cancer in the 7 years. Figure 1 shows the age distribution. The age group 0 to 5 years was the most affected accounting for 21 (58.3%) of the cases. The youngest patient was aged 5 months ( Figure 1). Twenty three patients were males and 13 were females. (Male: female ratio = 1.8: 1). Table 2 shows the distribution of cancers according to age groups. The 0 – 5 year age group accounted for 21 (58.3%) of the cases. The commonest malignancy in this age group was Burkitt’s lymphoma. Burkitt‘s Lymphomas were accounted for a third (33.3%) of the tumours in the 0 – 5 age group (Table 2). The commonest type in the 6 – 10 years age group was non Hodgkin’s lymphoma. In males, Burkitt’s lymphoma accounted for 14 (60.9%) of cancers while in females the tumours were more evenly distributed (Table 3). Table 4 shows the location of the cancers. Most tumours were located in accessible sites for the guardians or patients as well as the health workers. Clinical features on the 5 main cancers were many. A swelling or mass was the predominant presentation. Other features included pyrexia, peripheral lymphadenopathy, hepatomegaly, splenomegaly, weight loss, pallor and abdominal tenderness. Others signs and symptoms deferred from one type of cancer to the other. The site of tumour varied. Burkitt’s lymphoma was located in maxilla and mandible (8 cases over 10:80%). Thirty four patients had confirmed histological diagnosis. Two patients had diagnosis confirmed by bone marrow examination. Tables 6 and 7 summarize the mode of treatment received by the children. One form of surgery or the other was performed in 17 (47.2%) of the patients and included tumour excision, limb amputation, Nephrectomy, eye exenteration and others. Only 4 patients (11.1%) benefited from chemotherapy. Palliative treatment was offered to 13 patients with advanced disease. Palliative care included analgesics, intravenous fluids, blood transfusion, and nursing. Radiotherapy is not offered in Rwanda and therefore none of the patients had such a modality of treatment. Only 4 patients had chemotherapy. Two patients with NHML received a combination of Endoxan 40mg /m2 + Vincristine + Methotrexate + Prednisolone for 2 sessions. One patient with Burkitt’s Lymphomareceived 3 sessions of Endoxan 40mg/m2 and Prednisolone 2mg/ kg. One patient with Acute Lymphoïd Leukemia had Endoxan 40mg/m2 + Vincristine1,5mg/m2 + L-Asparaginase+ Methotrexate + Prednisolone 2 mg/kg. The average length of stay in hospital was 36.6% days with the extremes of 2 days and 510 days. Table 1. Patients’ Distribution According to Years of Admission.
Table 2. Age Distribution and type of cancer.
*NHL = Non Hodgkin Lymphoma, **Ac LL = Acute Lymphoïd Leukemia Table 3. Patient Distribution According to Type of Cancer and Sex.
*NHL = Non Hodgkin Lymphoma, **Ac LL = Acute Lymphocytic Leukemia Patients’ complications were: infection, bonemarrow aplasia, blindness, nausea, vomiting, observed in 4 (27.7%) patients who had Burkiitt’s Lymphoma, acute leukemia or Hodgkin lymphoma under chemotherapy. The outcome at discharge varied: 11 patients (30.5%) improved, 15 patients (41.6%) didn’t improve that is general state remained the same or worsened. Ten patients died in hospital (27.8% mortality) and included 1 patient who had surgery, all 4 patients treated with chemotherapy and 5 patients managed with palliative care alone. The patients’ follow up was difficult, only 3 patients over 36 was seen 1 month later. Table 4. Sites of Cancers.
Table 5. Histological Types of Cancer in Children
Table 6. Patients Distribution According Treatment
Tableau 7. Patients outcome versus type of cancer
*NHL = Non Hodgkin’s Lymphoma **HL = Hodgkin’s Lymphoma Discussion Cancer is a subject of constant preoccupation in the world1. It is rare in children aged less than 15 years, it represents 1-3% of all tumors in the population2,3,4,5,6,7. In France, each year 1800 to 2000 new cases of cancer in children are registered1,3,8. In Switzerland, 220 children; in Belgium less than 300 children are affected each year. This study confirmed that cancer in children is a rare . Our hospital prevalence was similar to that reported by other sauthors3,5,6,9. The disease predominantly affects young children in the 0 -5 years age group. Other studies have reported similar findings.1,2,6. The clinical presentation in our children was in agreement with previous literature10,3,7,11,12. The patients’ management and outcome in our series significantly differed from what is reported by other centres with established surgical oncology departments1,3,5,13. In our study, surgical treatment, being the only available form of treatment for cancer in the country, was offered to many cases.. Antimitotics drugs were not always available, and they were too expensive for ordinary Rwandese patients. There is no Radiotherapy Centre in the country nor is there any well established chemotherapy unit. This unfortunate situation contributed to the poor outcome and bad prognosis of our patients. The need for establishing such centres in the country is overwhelming. Conclusion Our findings showed that the clinical features and pathological types of cancersseen among children in Rwanda were similar to what has been reported by other authors in the literature. But the difference was that most of our patients were admitted in advanced stage of the disease. Because of lack of an Oncology Department, absence of appropriate drugs for chemotherapy, and lack of radiotherapy and palliative Medicine, our patients’ management and outcome were poor. There is an urgent need to improve our Hospital in establishing proper structure and facilities to attend to cancer patients efficiently. Recommendations
References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08010f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}