 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 77-83 Open Fractures I Rwanda: The Kigali Experience. E. Twagirayezu, J.M.V Dushimiyimana, A. Bonane Kigali University Central Teaching Hospital, Kigali – Rwanda. Code Number: js08013 Background: Open fractures
are an important cause of morbidity and mortality. Their severity depends on
Gustilo grading which is based on degree of soft tissue destruction,
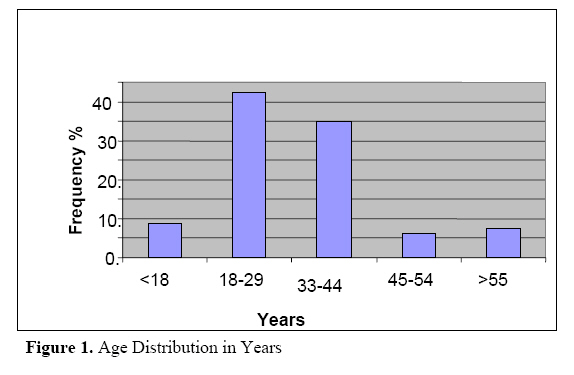
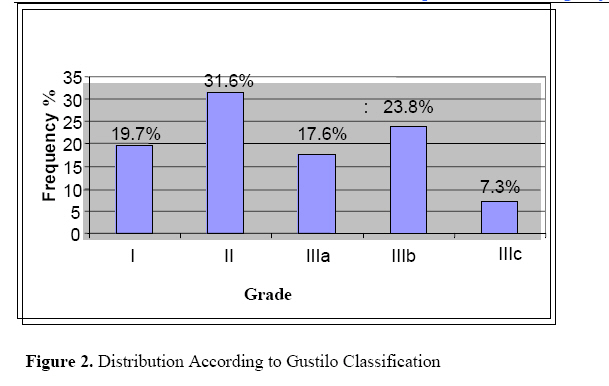
contamination and neurovascular state. Introduction Open fractures are a major and common public health problem that keeps the Orthopaedic/Trauma surgeons pre-occupied. They usually have adverse effects on the economy of the patients. Often, open fractures are due to severe trauma and result in deaths or grave sequelae. Their severity depends on Gustilo grading which is based on degree of soft tissue destruction, contamination and neurovascular state. Initial management constitutes a principal step which has to be early and complete. After resuscitation, toilet and debridement of wound are followed by stabilization of the bone and skin closure. Patzakis et al1,2in USA, found that early administration of the right antibiotic reduced the risk of infection by 14 – 20 %. Cauchoix et al3 showed the importance of appropriate initial treatment, its absence resulted in evolution complication with infection to soft issue and bones. In his study, Nzeyimana4 found that 82.7% of leg fractures were open. In another study from Rwanda, between 2001 and 2003, Rukundo5 observed that out of 279 fractures, 83.1% involved the lower limb. Limb open fractures constitute also the pre-occupation to the Kigali University Teaching Hospital (CHUK) traumatology unit. This study describes our experience with open limb fractures at CHUK traumatology unit. Methods This was a retrospective descriptive study that included all patients that were hospitalized with open fractures of lower limbs in the department of surgery of CHUK from 1st Jan 2004 – 31st Dec. The patients’ ages, sex distribution, causes, the sites of fractures and mode of management and its outcome were recorded and analyzed. The findings are presented Results During the period under review, 3088 patients were hospitalized in CHUK Surgery Department of which 192 (6.22%) presented with one or more open fractures of lower limbs. One patient who died as a result of poly trauma was excluded from the study. The results presented are based on the findings among the remaining 191 patients with 193 fractures. The mean age is 31 years. The majority (77.4%) of the patients was in the 18 – 44 years age group. The 18 to 29 age group contributed 42.4% (Figure 1). Males accounted for 77% of the cases giving a male to female sex ratio of 3.3: 1. The commonest cause was road traffic trauma recorded in 71.5% of lower limb open fractures. Other causes included falls in 9.3% and ballistic injuries in 5.7%. Fractures of tibia and fibula and of the femur contributed 69.4 % and 17.6% respectively. Using Gustilo’s Classification, 31.6% of fractures were grade I and II, 19.7% being grade I. Grade III were 48.7% of which 17.6% were Grade IIIa, 23.8% Grade IIIb and 7.3% Grade IIIc (Figure 2). Comminuted fractures with musculo-cuteneous lesions of Grade III had a high rate of complication and were difficult to treat. A total of 71.5% of our patient had treatment initiated within 24 hours. The average duration of treatment was 5.36 days with a STD of 10.8. Delay in starting treatment had a significant negative effect on the outcome of management; the longer the delay the more the complication especially infections. In 5.7%, no wound toilet or debridment was done and 16.1% of cases received no tetanus prophylaxis. The antibiotics prescribed were in the family of lactamine (cloxacilline, ampicilline, benzylpenicilline), derivatives of imidazoles (Metronidazole) and the phenicoles (chroramphenicol). A single antibiotic was given in 66.8% and in combination in 28% of cases. For the immobilization of the fractures, the plaster of Paris (POP) was applied in 32% of cases followed by external fixators in 31.6%. In our study, the femoral fractures patients were managed with traction followed by plaster cast in 38.2% and by intramedullary nailing in 35.3%. The fractures of tibia were treated with external fixators (EF) in 40.6% and plaster cast in 45.4%. The fractures of ankle joint and foot bones were treated with pins and plasters. Fifty (25.9%) of the 193 fractures had complications with infection alone being recorded 74%. The progression was influenced by size of wound, method of stabilization and time of treatment. The fractures stabilized with EF had more statistically significant complications (p-value = 0.009). Delay of treatment was associated with a high risk of complications (pvalue = 0.042) with higher rate of infection (p-value = 0.021). Discussion Open fractures most commonly affected the active population. In our study, 18 – 44 years age group accounted for 77.4% which was higher than the 65.3% reported by Moyikoua et al6 in Brazzaville. The average age in our series was 31 years compared to the 33 year found in Brazzaville. Males accounted for 77% in CHUK with sex ratio of 3.3: 1. The corresponding figures for males in Brazzaville were 72.8% and 66.7% in Nigeria67. The males were also found to predominate by Iken et al7 in Nigeria with a rate of 66.7%. Bonnevialle et al8 in Toulouse in France found the male sex predominance of 73.4%. The male predominance can readily be attributed to their being more involved in road traffic travel, violent sports, occupational accidents and wars. In this study, the commonest cause of open fractures was road traffic accidents recorded in 71.5% of lower limb open fractures seen in CHUK. In their review, Cozma et al9 in Italy and Fal et al10 in Abidjan found road traffic crashes to cause compound limb fractures in 74.1% and 67.3% respectively. Bonnevialle et al8 in Toulouse reported a higher figure of 81.6% being due to RTA. In Nigeria road traffic injuries were associated with open limb fractures in 55.5%5. Kotisso11 in Ethiopia found RTA to be a cause in 47.2% of open limb factures. Open limb fractures involved the leg bones in 69.4 % of the cases compared to the 17.6% for the femur. Moyikoua et al6 in Brazzaville found the rates to be 63.9% for leg bone fractures and 16.4% for femoral fractures. Ikem7 in Nigeria found the rates to be higher for leg fractures 79.6% and 20.4% for femur fractures. The leg bones are more predisposed to open fractures due to poor muscular coverage of tibia1213. In our study, the open limb fractures were classified as Gustilo grade I in 19.7% and grade II in 31.6% of cases. A total of 48.7% were Grade III with 17.6% being grade IIIa. 23.8% as grade IIIb and 7.3% as grade IIIc. In their series, Kotisso et al11 found grade II to account for 37%. In Brazzavile grade II open fractures were recorded in 48.7% of cases6. The size of the open wound influences the evolution of the fractures. In our study comminuted fractures with musculo - cuteneous lesions of G III presented a high rate of complication difficult to treat. Treatment The management principles are well established. The start of treatment should be as early as possible and should include anti-tetanus prophylaxis, surgical toilet and debridment, control of infection and fracture immobilization. Analgesics are also indicated. The surgical intervention should be within six hours of the injury. In our study 71.5% had treatment initiated within 24 hours. This was very good considering the many steps patients had to go through before being referred to the national referral hospital. Other patients had to wait for over 24 hours before definitive management that involved a back slab plaster (15.6%), or skeletal traction (12.9%). The average time before final surgical intervention was 5.36 days with a STD (ecart. Type) of 10.8. This delay was explained by lack of enough personnel more so orthopedic surgeons; lack of enough materials and the fact that other surgical emergences such as acute abdomen had to be given priority. At CHUK the same surgeon on call treats general as well as orthopedic cases. Delay in starting treatment had a negative effect on our results. The longer the delay is, the more likely to develop complications, especially infections. Open fractures are potentially infected. In our study, the antibiotics utilized included the family of b-lactamine (cloxacillin, ampicillin, benzylpenicillin), derivatives of imidazoles (Metronidazole) and the phenicoles (chroramphenicol). A single antibiotic was given in 66.8% and in combination in 28% operated cases. Patsakis1 found in 62.1% of instances, microorganisms could be treated by one antibiotic. Gustilo14 confirmed that early treatment with a broad spectrum antibiotic combined with toilet significantly decreased frequency of infection from 12% to 5% .Ikem et al7 in Nigeria found Staphylococcus in 61% of open fracture wounds, gram negative organisms (e.g. proteus mirabilis, P. aeruginosa) were isolated in 39%. These bacterio were sensitive to a combination of cloxacillin and gentamycin. Patsakis and Wilkims1 in USA recommend the use of active antibiotics to gram negative and gram positive. In their study, the infections which followed treatment with penicillin was reduced 5 times by cephalosporins. Unfortunately the cost limits their utilization especially in the poor nations of over the world. Brown et al16 recommend the addition of anti-anaerobic antibiotic in case of a large open wound. Moyikoua et al6 in Brazzaville found the rate of infection to be 26.6% irrespective of early treatment and systematic use of penicillin and their derivatives. In other studies the rates of infection were 33.1% in Nigeria7 and 4.3% in Abidjan10. Stabilization of the bone In our study plaster was the most utilized (32%), then external fixators (31.6%). This is because open fractures of Gustilo I and II classes are more numerous: quite 50% of cases. In the study by Moyikoua et al6, closed treatment was utilized in 64.7% of patients and recorded a risk of infection of 26.6%. Closed treatment is a convenient type of treatment in the developing countries because it is cheap, non-invasive and with acceptable functional results. External fixators remain the most utilized in Gustilo III grade. There is a statistically significant relationship between the Gustilo class and the therapeutic method6710. In our study this relationship was confirmed. Plaster was utilized in classes I and II. Class IIIa and IIIb benefited from external fixation and for IIIc patients, amputation was performed in 57.1% of cases. The treatment of open limb fractures also depends on the site of fractures. In our study the femoral fractures patients benefited from traction followed by plaster cast in 38.2% and intra-medullary nail (IMN) in 35.3%. The fractures of tibia were treated with External Fixators in 40.6% and plaster in 45.4%. The fractures of ankle joint and foot bones were treated with pins and plasters. This variation in treatment which depends on the fracture site was also found in other studies 6,7,17,18. A relationship between the method of stabilization and evolution was evidenced in our study. A total of 42.2% of those managed with external fixators (EF) developed infection. This is understandable because EF is utilized in Gustilo III fractures with very large open wounds which are contaminated; the risk of infection is high. The method of stabilization also affects the duration of hospitalization. In fact all the tractions, 54.1% of EF and 40% of IMN spent over 4 weeks in the hospital. Bonneviale8 at Toulouse, France noted also that femoral fractures treated by traction spend more than 10 weeks in the hospital. Several studies have compared the various methods of stabilization of open fractures. According to Gustilo and Anderson14 EF should be used for all fractures with wound which are not easily accessed for dressing. Brumback19 and Selgiso and Henry18 observed that EF constitute the treatment of choice for open fractures and that internal fixation, should be reserved for Gustilo I + II where infection risk is said to be low. Cozma et al9 in their study on open fractures in Italy, found the rate of infections to be 13.8% for external fixators and 9.1% for intra-medullary nailing. Poor consolidation (Malunion) was found in 15.7% in EF against 5.8% in IMN. The IMN therefore has more advantages7. Gopal et al20 in their study comparing EF and internal fixation on Gustilo IIIa and IIIb with possibility of wound closure, the rate of infection was 13.1% with internal fixation compared to 37% for external fixation. In our study the IF was preferable in Gustilo I and II. Unfortunately, many of the patients in CHUK came late and had to be treated for infection rather than prevention of it. For Gustilo III, EF remains the treatment of choice. Outcome of treatment. In our study, 50 (25.9%) out of the 193 fractures, had complications with infection alone accounting for 74% of the complications. The outcome was influenced by the size of wound, method of stabilization and time of treatment. In this study the rate of complications increased with advancing grade of Gustilo, resulting in 42.9% of Gustilo IIIc open fractures developing complications, the chi-square test gave a significant value of 0.047. This influence was also noted by Chapman and Mahoney21 their study on early I.F. of open fractures in limbs. They obtained an overall complication rate of 10.6% being 21% in Gustilo III21. Staggs et al22 re-affirmed this finding in their study on outcome of open fractures in infants. The infection rate depended on the grade of Gustilo with a an overall rate of 18% in grade III. Gustilo et al15 in USA reported a complication rate of 13.7% for grade III open fractures. Our study revealed that the fractures stabilized with external fixation had more complications. This association was statistically significant with a pValue of 0.009. Similar findings reported by Gopal et al19. In our study, we found a statistically significant association between delay in treatment and risk of developing complication (p = 0.042). Conclusion
References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08013f2.jpg] [js08013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}