 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 95-100 Splenic Injuries in a Semi Urban Hospital in Nigeria E.A Agbakwuru, A.A Akinkuolie, O.A Sowande, O.A Adisa, O.I Alatise, U.U Onakpoya, O. Uhumwango, A.R.K Adesukanmi. Department Of
Surgery, Obafemi Awolowo University, Ile-Ife. Nigeria Code Number: js08015 Background: The management of
splenic injury has changed dramatically over the last two decades. The
objective of this study is to evaluate splenic injuries in our community and
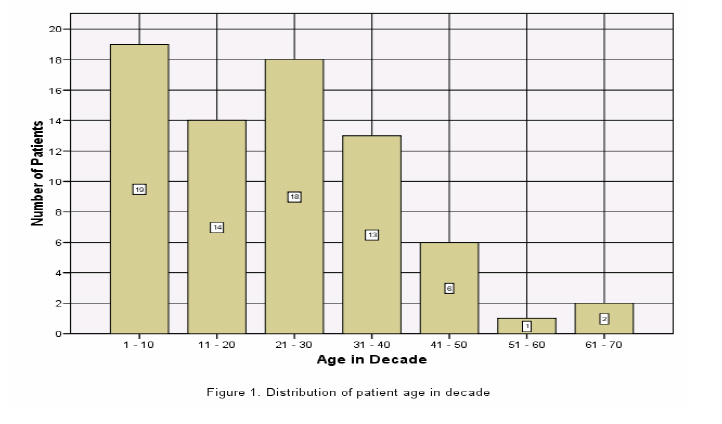
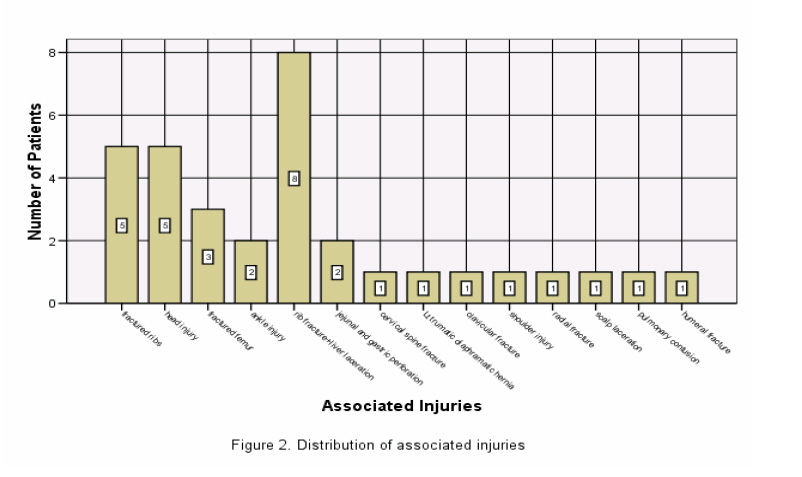
factors affecting the outcome of treatment modalities. Introduction Splenic injuries occur worldwide both in developing and industrialized countries. The common causes include road traffic accidents, fall from height, penetrating injuries such as gunshot and stabbing1,2.Following the first successful total splenectomy in the 16th century, total splenectomy came to be regarded as the main mode of treatment for splenic injuries; however, with the recognition of increased incidence of systemic infection following splenectomy by encapsulated organisms: and soon after the understanding of the immunological as well as the anatomy of the organ, the treatment of splenic injury shifted from total splenectomy to splenic preservation3,4. This can be achieved by conservative means, angiography and embolization or operative salvage. Operative salvage can be by splenorrhaphy, partial splenectomy, subtotal splenectomy or deliberate autotransplantation5,6. The treatment method employed depend on the grade of splenic injury, heamodynamic stability of the patient, associated injuries, anaesthetic technique, laboratory back-up and the experience of the surgeon7-9. The objective of this study was to evaluate splenic injuries and to determine the factors affecting the outcome of treatment modalities in Obafemi Awolowo Teaching Hospital Complex (OAUTHC), Ile-Ife. This hospital is located in the South-western part of Nigeria and serves the health needs of three neighbouring States. Patients and Methods A prospective descriptive study of 73 patients treated for splenic injuries in our surgical unit between 1991 and 2006 was carried out. The patients either presented directly or were referred to the accident and emergency unit of OAUTHC from peripheral hospitals. They were initially reviewed by the medical staff in the Accident and Emergency unit before being referred to the general surgical unit The age, gender, cause of injury, associated injuries, blood pressure at presentation, sonograhic grading, intra-operative grading using America Injury severity grading system (AIS), amount of haemoperitoneum, blood transfusion requirement, treatment modalities, outcome, post operative and follow-up complications were entered in the proforma designed for the study. All the data were analyzed using SPSS 13 software for windows using descriptive statistics and linear regression with significant level put at p < 0.05. Results The patients’ ages ranged from 3 to 65 years with a mean of 24.2 ± 15.2 years. There were 50 males and 23 females giving a Male: female ratio of 2.2:1. The highest incidence was in the first decade with 19 patients followed by 3rd decade with 18 patients: the distribution is as shown in Figure 1. Blunt injuries accounted for 95.9% of the cases. Road traffic accident accounted for 55 (75.3%) of the injuries. Other causes were falls from height 10 (13.7%), gunshot injury 3 (4.1%), assault 2 (2.7%), child battery 1 (1.4%), domestic injury 1(1.4%) and sport injury 1 (1.4%). Thirty four (46.6%) of the patients presented with grade IV splenic injury, 19 (26%) with grade III, sixteen (21.9%) with grade II, 3 (4.1%) with grade V and one (1.4%) patient with grade I splenic injury. Thirty three patients had associated injuries; the commonest being rib fracture with liver laceration The pattern of associated injuries was as shown in Figure 2 Road traffic accident accounted for these associated injuries in twenty-nine patients of which 60.6% had grade IV splenic injury. Fifty-five patients had their injuries from road traffic accident, 28 (50.9%) with grade IV, 11 (20%) with grade III, 13 (23.6%) grade II and 3 (5.5%) with grade V. None of the patients presented with grade I splenic injury. The most common associated injury in the road traffic group was rib fracture with liver laceration seen in 8 (14.5%) followed by head injury in 5 (9.1%) of the cases. Of the 73 patients, 53 (72.6%) had splenectomy and 20 (27.4%) had splenic preservation. Of those that had splenic preservation, 5 (6.8%) had non operative treatment, 14 (19.2%) had splenorrhaphy and one (1.4%) had partial splenectomy. All the patients with grade IV and V injuries had splenectomy. Only 13 out of 35 patients with grade II and III injuries had splenorrhaphy; the rest had splenectomy. All the 5 patients that were managed conservatively had grade II splenic injury. Overall, there were post operative complications in sixteen patients (21.9%). These were due to development of wound infection in 5 (6.8%) and respiratory distress syndrome in 3 patients (4.1%). Other postoperative complication recoded respectively in 1 patient (1.4%) each were pneumothorax, subphrenic abscess, pulmonary embolism, extradural haematoma, acute renal failure, reactionary haemorrhage, stitch sinus and malaria. There were 8 deaths out the 73 patients treated which gave an overall mortality of 10.96%). All the mortalities were in multiply injured. Sixty three 63 (86.3%) of the 73 patients were discharged with good outcome, one patient was referred for the management of her extradural haematoma which developed 6th post operative day and the remaining one patient was discharged against medical advice while undergoing conservative management of her splenic injury. The factors that significantly affected patients’ recovery and good outcome were (Table 1):
The follow-up periods ranged from 2 weeks to 7 years, with a mean of 11.9 months with 35 patients being lost to follow-up. During the follow-up period, 3 patients presented with hypertrophic scars, one developed adhesive intestinal obstruction, one patient with recurrent malaria and another patient with incisional hernia. None of these patients presented with overwhelming post splenectomy sepsis Table 1. Factors affecting patients’ Recovery
P < 0.05 Discussion The spleen is a commonly injured organ in intra-abdominal trauma second only to the liver. The commonest cause of injury being vehicular accident and this is usually blunt in majority of cases10, 11. The mean age of patients in this study was 24.2 years with the highest incidence between the second and third decade which is similar to findings by Obekpa12 in northern Nigeria in 1997. The male: female ratio in this study was 2.2:1. The majority (75.3%) sustained their injuries following vehicular motor accident; 95.9% of these were due to blunt trauma to the abdomen. This was comparable to the experience of Al-Qahtani10 in Saudi-Arabia. Twenty-nine (87.8%) out of the thirty-three patients with associated injuries also had their injuries from vehicular motor accident and 60.6% of these patients had grade IV splenic injury which is a reflection of severity of the accident and the degree of energy impart. This vehicular cause of injury is preventable or can be minimized by reducing the amount of energy transferred to the occupants by ensuring strict compliance to the local road rules. The abuse of alcohol, driver fatigue and non-compliance to the principles of driving may play major role in the aetiology of these accidents13. Improvement in road conditions, prevention of overloading of commuter vehicles and vehicle design changes with minimal safety standards will decrease the frequency and extent of these injuries13,14. The high degree of associated injuries also underscores the need for multidisciplinary care of these patients: with inter-specialty coordination where necessary with a view of early management and this will also eliminate duplication of theatre time14. Twenty (27.4%) of the 73 patients had splenic preservation out of which only five (6.8%) had non-operative management. This in contrast with communities with well developed health care system where reported cases of non-operative management of blunt splenic injury approaches 70%15. In communities with developed health system, availability of adjuncts to non-operative management of splenic injury improves their rate of splenic conservation; the developing nature of our health system and haemodynamic instability of these patients on presentation makes operative management inevitable. Operative salvage rate of 20.6% in this study is equally low because of high incidence of associated injuries and large percentage (50.7%) of these patients presenting with grade IV and V splenic injuries. All the eight mortalities had operative treatment and they died from their associated injuries which is similar to the findings by Franklin et al15 in their review. The post operative complications except for stitch sinus and malaria were due to associated injuries and this does significantly not affect the outcome. The factors that significantly affect the outcome in this study included the age of the patients, cause of injury, accident and emergency systolic blood pressure, intra-operative blood transfusion and the amount of haemoperitoneum. It is of interest that none of these patients represented with overwhelming post splenectomy sepsis; though, thirty-five (47.9%) out the seventy-three patients were lost to follow-up: hence, it might be impossible to reach definitive conclusion. Conclusion Vehicular motor accident remains the commonest cause of splenic injury in our community with high rate of associated injuries and the need for inter-specialty care of these patients; age of the patient, cause of injury, accident and emergency systolic blood pressure, intra- operative blood transfusion and amount of haemoperitoneum are the factors that determines good outcome in this study. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08015f1.jpg] [js08015f2.jpg] | ||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}