 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
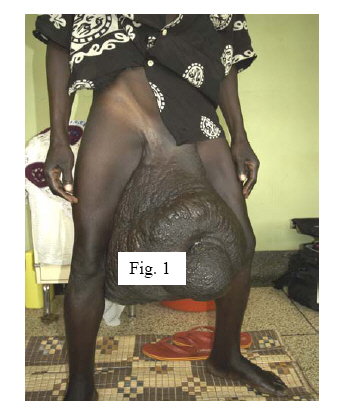
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 110-116 Giant Peno-scrotal Lymphoedema: Surgical Considerations and Management. Kalanzi E.W., Ssentongo R , Zeeman R Plastic and
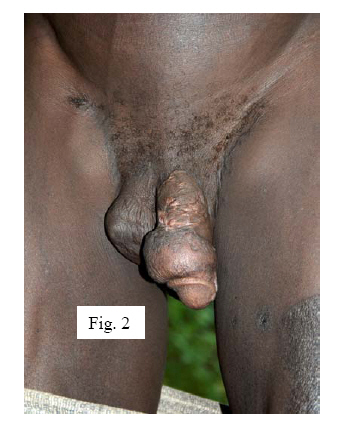
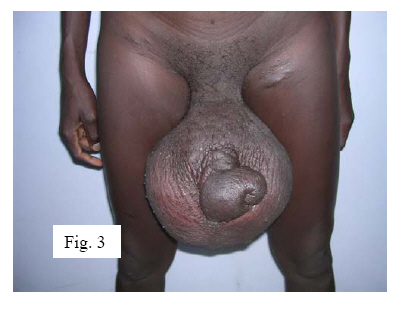
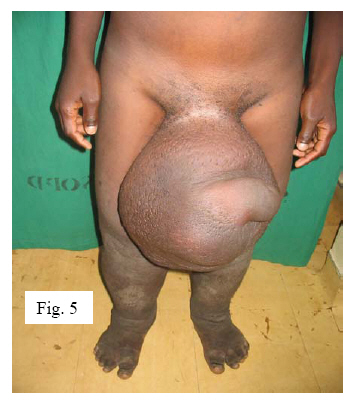
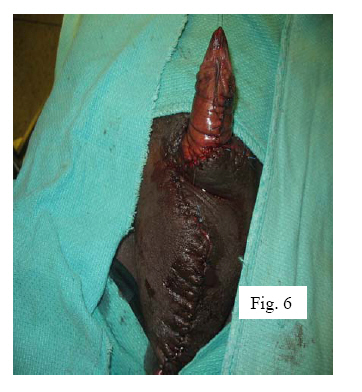
Reconstructive Unit Mulago Hospital, Kampala Uganda Code Number: js08018 Chronic lymphoedema can affect any parts of the body, including the scrotum and penis. Massive scrotal lymphoedema with gross genital deformation is called penoscrotal elephantiasis1. Penoscrotal elephantiasis can be a functionally and emotionally incapacitating dilemma to the patients. Usually patients suffer from pain, chronic irritation, repeated infections, ambulatory problems, sexual dysfunction and social dejection. Congenital (primary) lymphoedema is due to malformation of the lymphatic vessels and are rare conditions for example the congenital hereditary elephantiasis of the Meige type2. Acquired (secondary) genital lymphoedema can be caused by genital infection such as lymphogranuloma venereum (LGV), filarial infestation like Wuchereria bancrofti, recurrent inflammation, tumors, lymph node dissection, trauma and radiotherapy3. With severe penoscrotal lymphoedema, the mainstay of treatment involves surgical excision, followed by reconstruction using local flaps or skin grafts. We present 3 cases of giant penoscrotal elephantiasis treated by excision and reconstruction with anterior and posterior flaps as a successful treatment of this difficult problem. Case 1 O.M. a 38 year old male peasant farmer was admitted in the Plastic Surgery Unit, Mulago Hospital because of giant penoscrotal elephantiasis. He had been well until 15 years previously when he began suffering from bilateral swelling of the inguinal region associated with pain in the scrotal region. He sort treatment from a local health centre with only relief of pain. The swelling continued gradually over the years. He denied history of pus discharge from the penis or scrotum. He consulted various hospitals in his locality without success. At one time he got married but soon after his wife abandoned him because of his deformity. The scrotal swelling became so massive that he could only move by carrying it on a wheelbarrow! At that stage some good Samaritans got to know of his calamity and brought him to us. On examination, there was no evidence of extremity or truncal lymphoedema. He had massive scrotal lymphoedema measuring 70x45x40 ( Figure 1) making differentiation of anatomic structures impossible. The penis was completely invaginated within the scrotum. Two superficial decubital ulcers were found on dorsal aspect of the scrotum and severe skin changes were noted over the scrotum. Laboratory findings were not significant including the absence of microfilaremia The patient was taken to theatre were under spinal anaesthesia the massive penoscrotal lymphadematous tissue was resected. The major steps taken involved first to identify both testis and spermatic cords and preserve them, then through a longitudinal T shaped incision, the penis was identified at which point a Foleys catheter was inserted into the urethra to guide us in the exteriorsation of the penis without damaging it. The glans of the penis was preserved. Anterior and posterior flaps of normal appearing scrotal tissue were outlined and incisions were made to develop these flaps in the subcutaneous plane. A 42kg mass of chronic lymphadematous tissue was excised. After thorough haemostasis, the wounds were closed over two corrugated drains. The shaft of the penis was partially closed with its glans and the remainder with a thin thickness skin graft. Postoperatively the patient developed some sepsis which resolved with ceftriazone, clavulin and metronidazole. The final outcome of surgery is seen in Figure 2. @ years later the patient was doing well without any recurrence of lymphoedema. Case 2 A.K. a 16 year old Male presented to us with a massive penoscrotal elephantiasis. He had been well until 5 years previously when he developed progressive swelling of the inguinoscrotal region bilaterally. He sought treatment from a local hospital where the attending doctor did an inguinal node biopsy and diagnosed him to be having TB adenitis. He started him on anti TB drugs for one and half years. However the scrotal swelling continued to even involve the penis. At that point he `went to another hospital were he was treated for filariasis with invermectin and other non specified drugs. But still this did not alleviate his problem. At the time of presentation to us he had started having marked pain in the scrotum and difficulty in walking. He denied history of weight loss, penile discharge and fevers. He had normal micturition habits. On examination we found a young man with giant penoscrotal elephantiasis. The extremities and truck were free of lymphoedema; he had old surgical scars around both inguinal regions ( Figure 3. the scrotum measured 45x40 x38 cm, the penis was invaginated into the scrotum and difficult to palpate. The glans was positioned 25 cm from the cutaneous opening where one imagined the penis to be. There were marked skin changes over the scrotum.. Preoperative laboratory tests were basically normal. The massive penoscrotal mass of 20kg was excised as in the previous case report. The postoperative period was uneventful. Histopathological report showed marked fibrosis of scrotum with hypertrophied muscle, dilated lymphatics, thickened vessel walls, cells of chronic inflammation and oedema. The features were in keeping with chronic non specific inflammation. The patient was discharged from hospital in good general condition. Subsequent follow up showed a satisfactory result ( Figure 4 below) Case 3 B.P a 23 year old male peasant presented with a 10 year history of swelling of both lower limbs and penoscrotal region associated with difficulty in walking. He reported that prior to onset of the swellings he `developed a febrile illness which was treated with antimalarials and other nonspecified drugs at a local health centre. Gradually the swellings increased for both the legs and the scrotum. There was no associated pain, skin swellings in other parts of the body, neither itching, nor penile discharge. He sought treatment from various health facilities without relief to his problem. Clinically we found a young man with giant penoscrotal elephantiasis associated with marked bilateral lower limb elephantiasis ( Figure 5 above). There was an old scar in the left inguinal region though he had denied any surgical history.The penoscrotal mass measured 40x40x35 cm, there were marked skin changes and the penis was significantly deformed. Haematological tests were normal in particular no microfilariae were seen in his blood. Extensive resection of the penoscrotal tissue was done under spinal anaesthesia using the technique already mentioned above. The resected mass weighed 22 kg . In this case we were able to cover the whole penis using only the glans ( Figure 6). The Foleys catheter was removed on the seventh day postoperatively. Pathological examination of the specimen showed chronic non specific inflammation with lymphatic proliferation. The patient developed mild sepsis of the wounds which resolved with I.V. Ceftrazone and Ciproxacillin. He was discharged on the twelfth day postoperatively in good general condition. The patient was lost to follow up; we did not treat his lower limb lymphoedema. Discussion Lymphoedema results from the accumulation of protein- rich lymphatic fluid in the skin and subcutaneous tissues due to a dysfunction in the lymphatic system. Genital lymphoedema can be classified as congenital (primary) or acquired (secondary)4. Primary lymphoedema results from maldevelopment of the lymphatics and lymph node blockage and it usually starts at puberty. The secondary lymphoedema is caused by mainly filarial infections like Wuchereria bancrofti and Brugia malayi, tumors, irradiation, lymph node dissection and trauma. We were not able to ascertain the exact cause of penoscrotal elephantiasis in our miniseries but we thought it to be filarial infections since the patients were coming from endemic regions. Regardless of the lymphatic disruption, scrotal lymphoedema can be treated in similar ways. Diagnosis of scrotal lymphoedema may be made by lymphoscintigraphy. This technique uses radiocolloids to delineate the anatomy and functional point of obstruction within the lymphatic system.. Immunodiagnosis with indirect fluorescence can be used to detect the antibodies in case of filariasis in over 95% of cases1. Both these techniques are not available in our hospital. We depend on clinical diagnosis and at times wet preparations of body fluids and tissues in which the microfilariae can be seen with low power microscope. This is a less reliable technique as most of the microfilariae exhibit a nocturnal periodicity. Treatment of penoscrotal elephantiasis can be medical or surgical. The medical one is usually employed in the early stages to treat the diagnosed infection for example filariasis with Diethylcarbamazine. Also scrotal elevation with athletic support garments may be used to decrease swelling in the mild forms. With severe scrotal lymphoedema, the mainstay of treatment has been surgical excision, followed by reconstruction using local skin flaps or skin grafts. Ideally, the best treatment of lymphoedema would be restoration of the lymphatic system by microsurgical procedures such as lymph angioplasty and lymphaticovenous anastomosis which have been proven to be effective5,6. The use of anterior and posterior skin flaps to reconstruct the scrotum gives a satisfactory cosmetic result as seen in our miniseries. It preserves the scrotal anatomy better as the normal anterior scrotal skin is retained. Lateral skin flaps, fasciocutaneous thigh flaps can also be used to cover the testes7,8. If no normal surrounding tissue is available to form a flap, skin grafts can be used for the reconstruction9. The problem of using non scrotal tissue and skin grafts to cover the testes is that, it causes altered testicular thermoregulation and potential infertility10. This method has several distinct advantages: it removes all the lymphadematous tissue. It can be done in one stage, requires short hospitalization and we feel that it gives a good cosmetic result. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08018f2.jpg] [js08018f5.jpg] [js08018f3.jpg] [js08018f1.jpg] [js08018f4.jpg] [js08018f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}