 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 1, March-April 2008, pp. 116-119 Crepe Bandage in the Management of Soft Tissue Limb Abscesses A.A Akinkuolie1, O.A Oladele1, C.A Omotola2, A.O Adisa1, O.A Arowolo1, A.R.K Adesunkanmi1, O.J Kumuyi2 1Department Of Surgery, Obafemi Awolowo
University, Ile-Ife. Nigeria. Code Number: js08019 Objective: To determine the
necessity of continuous gauze packing of abscess cavities following incision
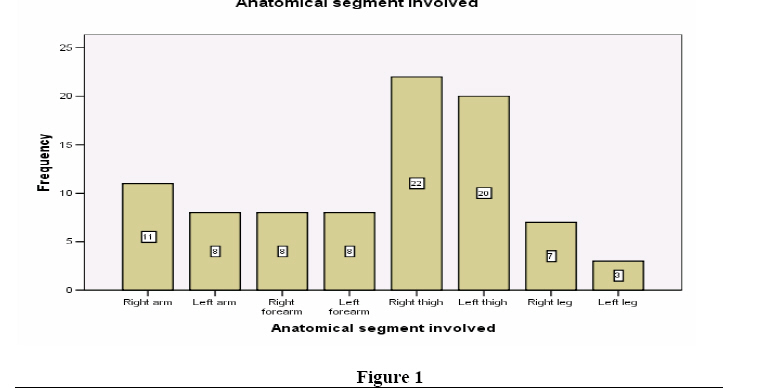
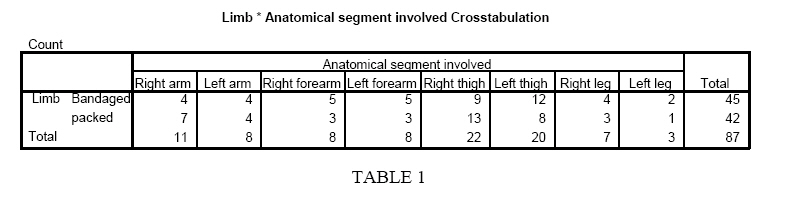
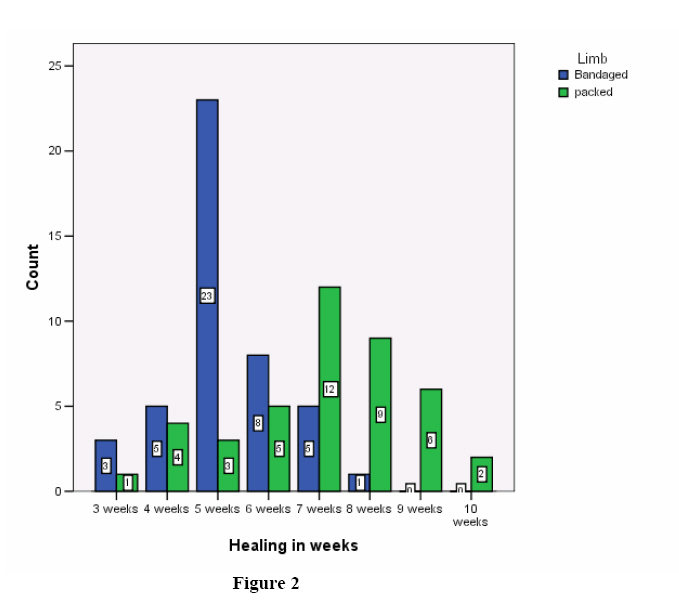
and drainage of limb abscesses. Introduction Limb abscesses are commonly encountered in tropical surgical practice1. Tropical pyomyositis, in spite of its name; is by no means limited to the tropics2. It accounts for the majority of cases of soft tissue limb abscesses3. The diagnosis is usually a clinical one, but confirming deep soft tissue abscesses and distinguishing between a purely soft tissue infections and underlying bone involvement may require radiological investigations such as plain radiographs, computerized tomography scans or a magnetic resonance imaging1, 3, 4. The goal of treatment is adequate drainage of the abscess, appropriate antibiotic, nutritional support and rest. Surgical drainage is most often required and involves wide incision along the long axis of the limb and splitting of muscles along the line of their fibers to access the abscess cavity following which the cavity is packed with gauze to prevent premature closure of the incision and drainage site and also to allow drainage5. The packing process is often associated with prolonged morbidity, severe pain during dressing, increased cost and the need for a secondary closure by direct suturing or with a skin graft. We therefore embarked on this study to determine if following incision and drainage of soft tissue limb abscesses, continuous gauze packing of the abscess cavity is really necessary in achieving ample healing; by determining if there is significant difference in wound healing time or the presence of other wound complications between wound treated by continuous packing and those not so treated. Patients and Methods A prospective study of 33 patients with abscesses in 87 limbs who were managed for limb abscesses over a period of five years between January, 2001 and December, 2005 at Federal Medical Centre, Owo, Ondo State, Nigeria, were carried out. 29 were in right lower limb, 23 in the left lower limb, 19 were in the right upper limb and16 were in the left upper limb: the distributions as shown in Figure 1. On admission, patients were resuscitated where necessary and they all had parenteral cefuroxime, anemia corrected in those that were anemic. The patients had drainage of their limb abscesses under conscious sedation through the most dependent part of the limb. The abscess cavities were lavaged with diluted hydrogen peroxide and eusol; specimen of the abscess sent for microscopy, culture and sensitivity. All wounds were packed for the first 24hrs for pressure homeostasis, after which the 87 limbs were randomized into two groups based on approximate equal volume of pus drained as shown in Table 1. The first group had daily eusol dressing with gauze packing down to the depth of the abscess cavity while the second group had daily eusol dressing of the stoma only with external crape bandaging of the abscess cavity. All the patients had more than one anatomical limb involvement which was so randomized. Parenteral antibiotics changed according to the sensitivity pattern and continued till the fever subsided after which oral antibiotic was continued for further 72hrs, none of them was malnourished. All wounds healed secondarily, none was skin grafted or require secondary wound closure. Outcomes were measured by the duration of wound healing and the presence of residual limb abscess. The wounds inspected weekly for healing and complications. Analysis was done using statistical package for social science version 13. The level of significance for independent-samples T test was put at p < 0.05. Results Eighty-seven limbs were studied in 33 patients; forty-five limbs were managed by bandaging and forty-two by wound packing: the distributions of limbs are as shown in Table 1. Nineteen patients were males while 14 were females with an age range of 9 years to 76 years and a mean age of 38.1 and standard deviation of 18.0 years. The mean duration for the gauze packed wounds to heal was 7.0 weeks with standard deviation of 1.08 weeks while the duration for the bandage wounds to heal was 5.2 weeks, with standard deviation of 1.71 weeks. The bandaged group heals faster than the packed wound as shown in Figure 2 which was statistically significant p < 0.000. There was one limb with residual seropurulent fluid in the bandaged group; this was managed by percutaneous aspiration. Discussion Open surgical incision and drainage is the traditional way of draining abscesses67, and these are often packed with gauze with wick drainage of the cavity; this is to prevent premature closure of the abscess cavity. Percutaneous drainage of deep abscess under ultrasonographic or computed tomography guidance89 are well documented as safe and effective but these are not readily available in developing countries like ours, hence the need for open traditional method. Packing of abscess cavity with gauze is a common surgical practice and easily managed by the nursing staff, but; it is usually associated with intense pain during change of dressing and with increase cost of the hospital bill in term of dressing materials. A statistically reduction in the time of wound healing was observed in the group of patients in who wound packing was avoided in this study, perhaps the process of continuous packing with gauze may delay the filling of the abscess cavity with granulation tissues. The impact of foreign body tissue reaction of the gauze packing on the process of wound healing is yet to be fully investigated. The repeated trauma of changing the gauze within the cavity, usually done daily may also have an effect on the process of wound healing; moreover, active muscles contraction against an external crepe bandage might provide better obliteration of abscess cavity than sequential gauze packing. In this study one limb in the bandaged group had residual abscess while the other 44 bandaged limb abscesses healed without any residual or recurrent abscess. Tokin etal7 in 2004 in a pilot study of 43 patients with perineal abscesses comparing packing with non- packing of wound cavities observed that, the mean healing times, rate of abscess recurrence and post operative fistulas formation were similar in the packing and non-packing groups. There is however paucity of literature on the subject about the need for packing of abscess wounds and our study among others should serve to stimulate further studies on the subject. Conclusion Continuous wound packing in limb abscesses apart from the first 24hrs to achieve heamostasis should be avoided, external crepe bandaging of the abscess cavity achieve better healing time while avoiding the undue pain of daily abscess cavity packing. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08019f2.jpg] [js08019f1.jpg] [js08019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}