 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
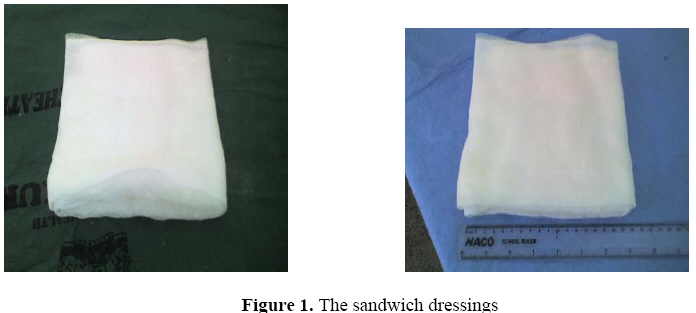
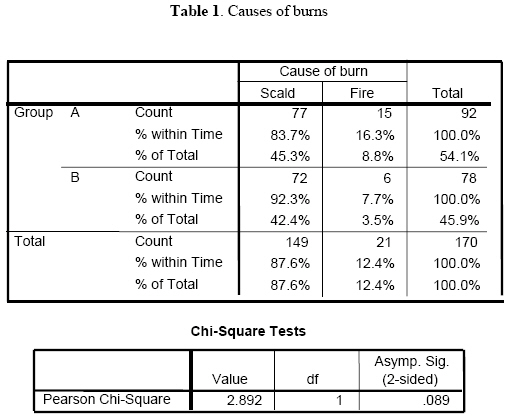
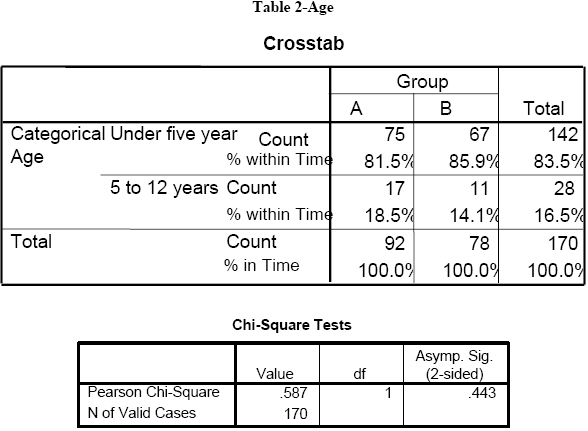
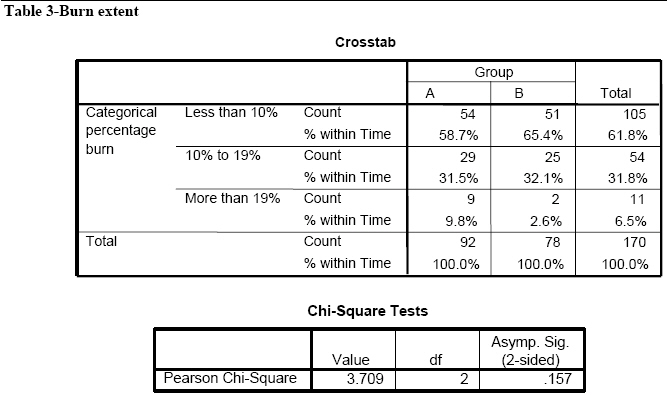
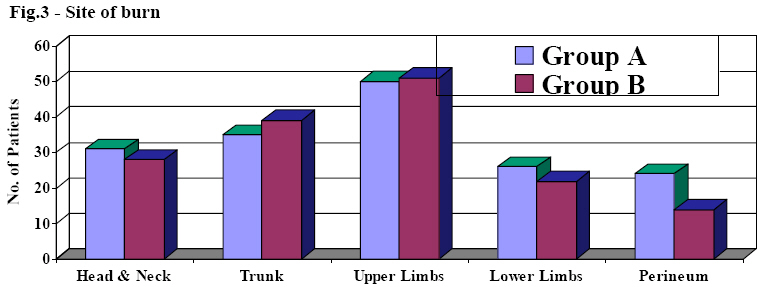
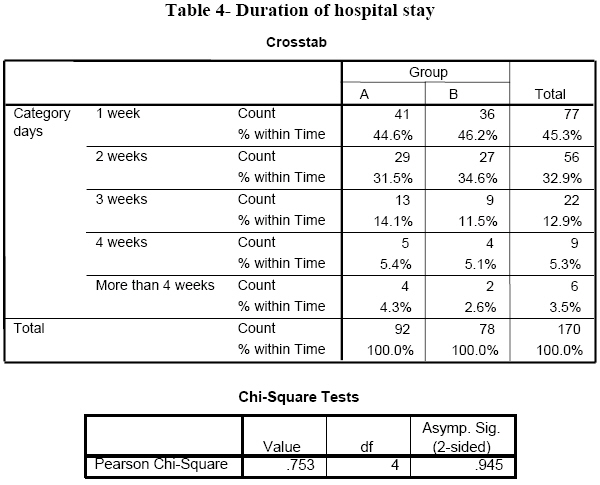
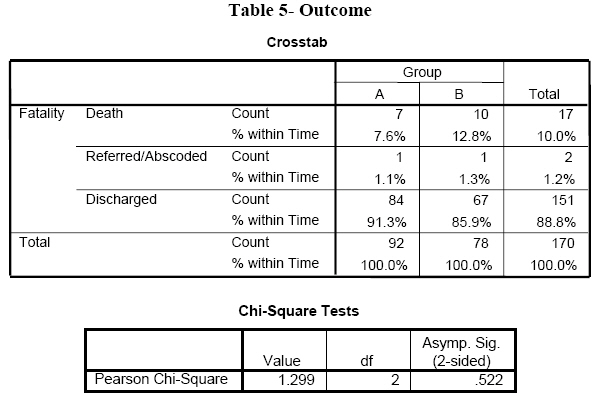
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 8-13 Open versus Closed Sandwich Wound Dressing Method in Burn Children P. Oduor, MMed Surgery, FCS(ECSA) Surgeon, Rift Valley Provincial General Hospital, Nakuru, Kenya. Email: Code Number: js08024 Background: Open method of dressing burn wounds has been the accepted mode of burn wound care in most of our hospitals. Closed dressing has been shunned because of the belief that it is costly and labour intensive. Introduction Burns are the most frequent injury among pediatric patients1. In addition, the long and painful scar treatment comes with significant financial burden for parents and society2. Burn care in Africa is very dependent on the availability of financial resources, equipment and expertise3. Burn wounds in Africa are treated according to the open method because regular dressing changes were found to be labor intensive and costly4. The dressing is sometimes left to the caretaker. The closed method of dressing burn wounds is now universally accepted for partial thickness burn wounds as it has less pain and also provides a moist environment which enhances wound healing5. It also allows for mobility of the patient. This method has been considered expensive because of the frequent dressing changes. The objective of this study was to find out if the closed method of burn wound dressing could be used in our set up. The sandwich method was used here where between two gauze layers is a layer of cotton wool to provide the bulky absorptive layer. The utilization of cotton wool for bulk reduces the amount of gauze required and hence the cost. From one roll of gauze about 17 pieces of this dressing material can be made (Figure 1). The dressing was applied after applying silver sulfadiazine to the wound. The dressing was maintained for between three and four days and only changed when the outer layer was wet (Figure 2). The ward where the study was conducted normally admits all pediatric surgical patients together with female adult burn patients. On average the ward admits 680 patients a year out of which 170 patients (25.7 %.) are pediatric burn patients. There is a perpetual shortage of nurses; hence the burden on them is heavy. The staffs have to take care of other patients besides caring for the burn patients. This picture is similar in most public hospitals across the region. To provide quality care a method of dressing not requiring daily changes would be ideal. Patients and Methods Medical records of pediatric burn patients (age less than or equal to 12years) admitted to the wards between June 2006 and March 2007 were reviewed retrospectively. In June 2006 to October 2006 the open method was being practiced while from November 2006 to March 2007 it was the closed method. Patient demographics, etiology, burn extent, anatomical areas, length of hospital stay and mortality were recorded. Statistical analysis of the data was performed using the SPSS statistical package. Results The patients treated between June 2006 and October 2006 were considered as Group A while the treatment group after October 2006 Group B. In both groups the most common cause of burns was scald (Table 1) with the age group affected being the under five years (Table 2). The total burn surface area in both groups was mainly 10% with a smaller group sustaining burns of between 10% and 19%.The mean was 10.32% for the open and 8.46% for the closed method (Table 3). The distribution of burn sites were similar with the commonest the being upper limbs and trunk (Figure 3). Statistical analysis of these parameters showed no differences when chi square was calculated. This could imply that despite the patients being treated at different time intervals they were affected in the same way. A total of 70% of patients in the open method of dressing stayed in the ward for two weeks while in the closed method it was 63% (Table 4).The mean duration of hospital stay was 11.07(10.17) and 10.13(6.97) respectively. 91.3% of the patients in the first group were eventually discharged against 85.9% in the second group (Table 5). The fatalities were 7.6% for the open dressing group and 12.8% for the closed dressing ones (Table 5). Once again there were no statistical differences between the two groups as far as the outcome indicators were concerned. Discussion The most common age group affected was the under 5years6,7. This corresponds to studies in other countries like Brazil, Ghana, China, and India where this age group was found to account for a disproportionately higher number of burns. Scalds constituted the commonest cause at more than 80% in both groups. This is the picture in most studies8,9,10. The TBSA in both groups was mainly 10% with a smaller group sustaining burns of between 10% and 19%.The mean was 10.32% (±8.23) for the open method and 8.46%(± 5.37) for the closed method. The distributions of burn sites were similar in both groups with the upper limbs and trunk being the commonest. This can be explained by the fact that children under 5 years and especially toddlers sustain burns as they reach objects as part of their curious nature11. A study at the University of Calabar Training Hospital, Nigeria had a different picture where the trunk was the commonest site12. The high incidence of burns in the trunk and limbs which are easy to dress makes this method amenable for use in most pediatric burns. Perineal and face wounds were not dressed using the closed method because of fear of contamination. Seventy percent (70%) of the patients in the open method of dressing stayed in the ward for a week while in the closed method it was 63%.The mean duration of hospital stay was 11.07(±10.17) and 10.13(± 6.97) days respectively. A study on 1494 pediatric burn patients in Shanghai, China found a mean hospital stay of 16.1(±12.2) days13 implying that our hospital stay was within the range of other countries despite utilizing the sandwich method with infrequent dressings; 91.3% of the patients in the first group were eventually discharged against 85.9% in the second group. Statistical analysis did not reveal a significant difference between the two outcomes. The mortality rates were 7.6% for the open dressing group and 12.8% for the closed dressing group. The higher figure for the closed method could have been due to teething problems since the method had just been introduced. However, no statistical difference was noted but the figures were high compared to the Shanghai, China study of 1.1%13. The mortality rate compared with an average of 9.9% found in many low and middle income countries14. Conclusion and Recommendations Closed dressing with dressing changes every three to four days does not adversely affect outcome of pediatric burn patients. The benefits of closed method of dressing can be gained by using this sandwich method. This method of dressing is affordable, has less pressure on nurses and also allows mobility of children in the ward. It is a method which can be useful in third world countries where resources are limited. Further studies will be required to see if the outcome will improve with time. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08024t4.jpg] [js08024t2.jpg] [js08024f2.jpg] [js08024t5.jpg] [js08024f1.jpg] [js08024t1.jpg] [js08024f3.jpg] [js08024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}