 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
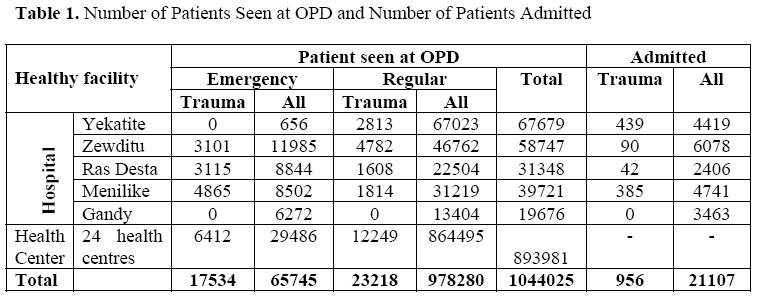
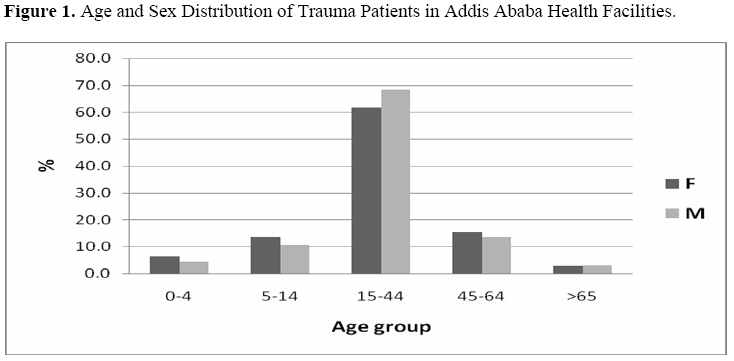
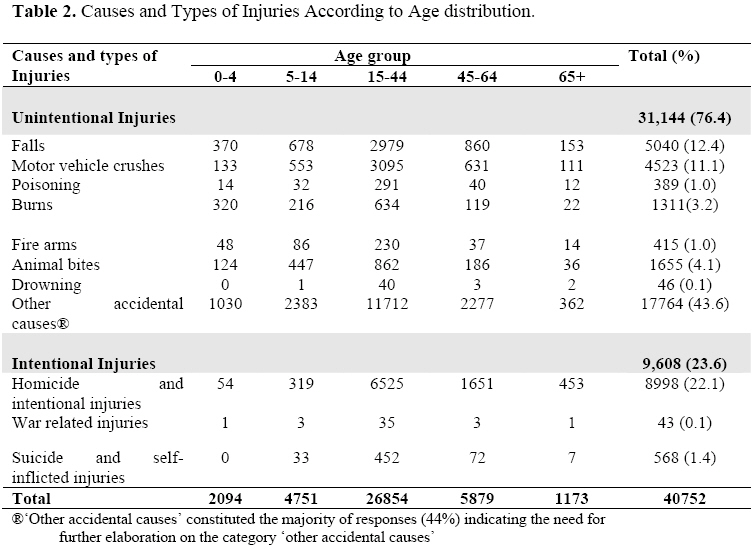
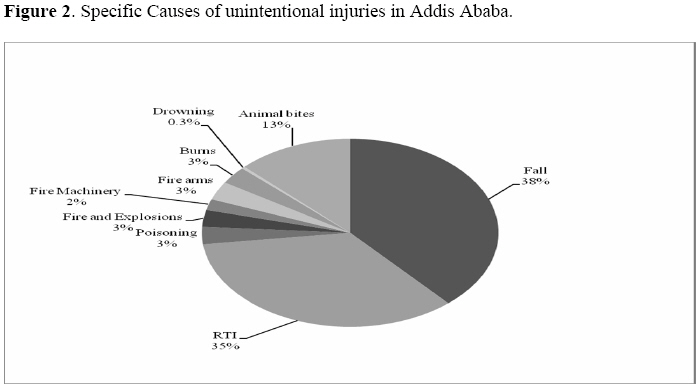
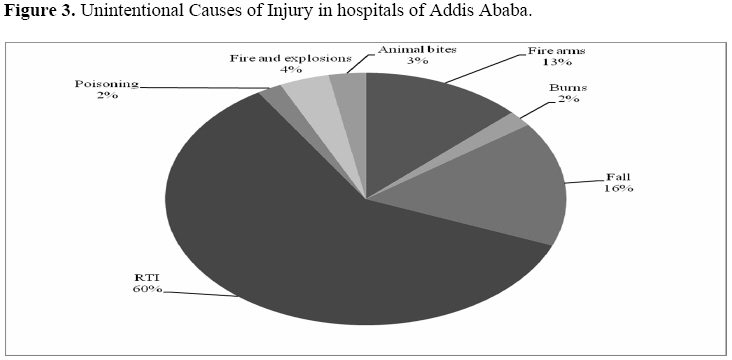
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 14-22 Pattern of Injuries in Addis Ababa, Ethiopia: A One-year Descriptive Study A. Wolde2, K. Abdella3, E. Ahmed 4, F. Tsegaye1, O. A. Babaniyi2, O. Kobusingye5, K. Bartolomeos6 1 Addis Ababa City Administration Health Bureau, P.O. Box 30738, Addis Ababa, Ethiopia Code Number: js08025 Background: Globally, trauma is recognized as one of the most life threatening public health problems. Traumatic injuries account for 12% of the global burden of diseases and are the third most important cause of overall mortality. This study was aaimed at assessing the burden of injuries in Addis Ababa, Ethiopia. Introduction Injuries are classified as unintentional and intentional (violence). Unintentional injuries comprise most of the traffic injuries, fires, falls, poisonings and drowning. On the other hand intentional injuries or violence are classified as interpersonal violence (including violence against intimate partners), collective violence (including war) and self directed violence (suicide). Globally, injury has been recognized as one of the most life threatening public health problems. Injuries represent 12% of the global burden of diseases and the third most important cause of overall mortality1. According to WHO, an estimated 5.06 million people die each year as a result of some form of injuries, comprising almost 9% of all deaths. This equates to almost 14,000 injury deaths every single day2. Millions of accidents occur each year and thousands of individuals lose their lives. This is well recorded in High Income Countries3-5. It was demonstrated that trauma patients occupied more than 12 % of hospital beds in the USA3 and accounted for more than 50% of orthopedic admissions in the UK6. For each death from injury there are many more injuries that resulted in either hospitalization, treatment in emergency departments, treatment by practitioners outside the formal health sector or never received treatment at all. The increased life expectancy together with urbanization and changes in lifestyle has lead to a rise in the incidence of non-communicable disease and injury in developing countries7-9. Injury is one of the commonest causes of death and disability in the African region, particularly among those aged 5-29 years. Three of the top five causes of death for this age group are injury related10. Every day in Africa, about 2,400 people die from injuries. Injury related deaths in Africa among people aged 15-44 rank second behind HIV/AIDS. For every person who dies of injuries over 35 others suffer from non-fatal injuries11. Road traffic injuries (RTI) are among the leading causes of injuries in Africa. Deaths from RTI in the African region are 40% higher than in all other low and middle income countries and 50% higher than the world average10. These injuries are an important and largely neglected health problem in developing countries12-17 . In Ethiopia, like other developing countries, injuries are common but little attention is being given to this problem18. Injuries constitute around a half of all surgical emergencies19, and were the major reason for an emergency room visit in Addis Ababa during 1999 (20), more than a quarter of all surgical admissions21-25, and 62% of orthopedic admissions in Black Lion hospital26. Data compiled by the ministry of health in 2000/2001 showed that injuries ranked fourth and fifth as a leading cause of admission and death respectively accounting for 6.2% and 1.6%27. Ethiopia hosts an annual road traffic fatality of 114 deaths per 10,000 vehicles and a property loss of over 56 million US dollars every year28. In Ethiopia the occurrence and health impact of injuries have not received due attention. This can mainly be attributable to the lack of information on the magnitude of the problem. The available scattered data has never been adequately collected, analyzed and transformed into accessible information to support informed interventions by the health planners. Our study was devised mainly to assess the burden of injuries in Addis Ababa. It was specifically designed to determine the pattern of commonly occurring injuries based on available healthy facility records. The review will make a basis for further regular data generation on the subject. Patients and Methods All new patients with external causes of injury and who had visited Health Facilities under the Addis Ababa health bureau between July 2005-June 2006 (equivalent to 1998 EC) were included in our audit. Patients who consulted more than once were excluded. The health bureau of Addis Ababa city administration is one of the biggest health bureaus in Ethiopia. Other than doing preventive health care activities, it also provide curative service in five hospitals ( Ras Desta, Minilik, Zewditu, Yekatit and Gandhi hospitals) and 24 health centers. All of the hospitals provide out-patient (emergency and regular) and in-patient services. Only two of the five hospitals provides all types of trauma services (one does not provide trauma services at all and in the other two no orthopedic related trauma services). Out of 927 beds in the five hospitals, 284 (30.6%) beds were for surgical and /or orthopedics. The health bureau is currently collecting routine health facility data using the District Health Information System (DHIS). The data reports on out-patient visits, discharges and deaths. Medical doctors filled out the charts of patients whereas data clerks compiled data using ICD 6 and entered the into the DHIS soft ware. Design: The data on injury for this particular audit was extracted from the DHIS. The data that include sociodemographic variables and diagnosis by causes, the condition of the patients at the time of their discharge for admitted patients were recorded. The injury related data (ICD codes 138, 139, 140, 141, 143-5, 147-9) were extracted from DHIS. Diseases were categorized according to International Classification of External causes of Injuries (ICECI) (29). Hospitalization or admission is defined as patients stayed in hospital beds and received treatment for more than 12 hours. The data analysis was performed with the aid of Microsoft excel software. Results were expressed in absolute numbers, percentage and ratio. Results A total of 1,044,025 patients were seen at the out-patient departments of health facilities under the health bureau of Addis Ababa city administration during the twelve months between July 2005 and June 2006, (equivalent to 1998 EC) of which 40,752 (3.9%) consultations were for injuries. New emergency patients accounfed for 65,745 cases while 978,280 were seen at regular out patient visits. Traumatic injuries accounted for 17,534 (26.7%) of emergency and 23,218 (2.8%) regular visits (31% of emergency and 10% of regular visits in hospitals and 22% of emergency and 1% of regular visits in Health centers) (Table 1). Socio-demographic Information Among 40,752 patients who had reported injuries, 25,528 (62.6%) were male and 15,224 (37.4%) were female giving a male to female ratio of 1.7:1. The majority of the patients, 26,854 (65.9%), were within the age groups of 15-44 years (Figure 1). Nine hundred fifty six (2.3%) patients were admitted, 552 (57.7%) were male and 404 (42.3%) female. Of all 21,107, hospital injury related admissions accounted for 956 (4.5%), ranged from 0-8.1%. Cause and Characteristics There were 31,144 (76.4%) unintentional and 9,608 (23.6%) intentional injuries. Forty four percent (17,764) were categorized under other accidental causes, details of which were not available (Table 2). Excluding all reported cases under the category of “other accidental causes” still leave the proportion of unintentional injuries relatively higher than intentional injuries, though the gap between the two becomes narrower ,13,380 (58.2%) versus 9,608 (41.8%). Falls were the most common cause of reported unintentional injuries seen and accounted for 37.7% of cases (Figure 2). Falls were exceptionally common in females aged over 65 years of in whom they were recorded in 52.2% of their injury related complaints. Overall, road traffic crushes (RTC) ranked second to falls as a leading cause of injury reported in a third (33.8%) of cases. Road traffic crushes were the top cause of injury in the age 15-44 years age group (Table 2). Animal bites were the third cause and contributed 12.4%. The dogs were responsible for 87.9% of animal bites. Other domestic or wild animals were involved in 12.1% of animal bite cases. Burns were ranked fourth (9.8%) but were the second commonest causes of unintentional injuries in children under 5-years. Of 9,608 intentional injuries, homicide and non-fatal interpersonal violence accounted for 93.7% of cases and suicide and self inflected injuries were found in 5.9%. Males were responsible for 6,491 (67.6%) of all reported causes of intentional injuries. Homicide and intentional injuries accounted for 5.4% of 6,845 injured children. Only six cases of deaths were reported at the out patient department in a year. Three thousand four hundred and seventy two (3,472) patients had visited the outpatient department at least twice, which increased the burden of work at outpatient department. The majority were injured by either motor vehicle 1,541 (44.8%) or fall 992 (28.6%). During the study period 956 injured patients were discharged, the reason for their admissions were unintentional injuries in 905(94.7%) of the patients and intentional in 51 (5.3%). Three hundred and eighty four (40.2%) of unintentional injuries were categorized under ‘other accidental causes’. Among specified unintentional causes, road traffic injuries were the leading causes of injury related admissions, accounted for 316 (60.7%) cases followed by fall 82 (15.7%) (Fig. 3). Among 956 hospitalized injured patients, the conditions of the patients at discharge were recorded for 696 (72.8%) patients, of whom the majority 653 (93.8%) were either improved or cured. Only 29(4.2%) patients had died during hospitalization. Fifteen of 29 deaths (51.7%) were as a result of road traffic crashes which gives higher mortality rate for road traffic injury related admissions 6.2% (15/241) (Table 3). Discussion Injury accounted for 27% of all emergency visit and 3% of all regular out patient department visits and 5% of all admissions. It was thought that large numbers of patients were visiting outpatient departments as a result of injury and occupying a large proportion of beds. This study did not find it to be true. However this impression probably resulted from the fact that first, many of the ´injured patients` visited a limited number of hospitals because of the availability of the service in those hospitals. Second, some of the hospitals included in our audit provide services only for specific types of injuries. Private hospitals have not been included in this study. The composition of our study population was similar to that found in developing countries, being a relatively young (age group of 15-44) and predominantly male, many of whom were likely to be heads of households and thus responsible for several family members16,19,30,31. More than three fourths of our injuries were unintentional in contrary to the other studies done elsewhere in North Gonder, Ethiopia19 and Jamaican injury profile32 where more than half is violence related but similar with injury experience of Black lion hospital , Addis Ababa30 and in Kampala33,34. A problem of violence against children does exist in Ethiopia. Falls were the leading cause of injury related morbidity accounting for 38% of all specified unintentional injuries across both sex and the two extremes of ages. The same finding was made in studies in Brazil and Thailand35,36. Road traffic injury is the second overall causes of unintentional injuries (first in age group 15-44 years) but it is the main burden of the health facility because it accounted for a) 34% of unintentional injuries, b) 45% of patients who visited the hospital twice or more, c) leading causes of injury related admissions (61%), and d) 52% of injury related deaths. Our audits are in agreement with the study in Addis Ababa (Black lion Hospital30), Kampala33,37, India38, China39, Pakistan40 and Italy41. The other surprising finding was the large number of patients bitten by animals especially dogs. Burns were the second leading cause of injury in children under five. This result is consistent with that of studies from other developing countries42-44. Ninety four percent of intentional injuries were due to interpersonal conflicts, men were implicated in more than two thirds of the cases. The results showed a high rate of misclassification. Forty four percent of all unintentional injuries were categorized under ‘other accidental causes’, indicating the need for further elaboration on this category which is not possible in the data available, Therefore we have deliberately excluded ‘other accidental causes’ during analysis. This was meant to avoid overrepresentation and misleading potential of this figure in the result interpretation. The status at discharge was recorded for only two thirds of discharged patients. There was unrealistically very low record of deaths from the out patient (only 6 deaths in a year). Given what previous studies in the same city had found (20 deaths at emergency OPD of Black Lion hospital in 6 months, this was considered to be very unlikely to be true30. Therefore, based on what were found to be incomplete records, it was very difficult to interpret the deaths in more detail. As it was shown by Wadman45 external causes of injury codes accurately describe the burden of injury derived from real patient encounters in specific geographic region which is true in our audit except that our data is suffering from misclassification and incompleteness. Critical to any injury prevention activities is a reliable surveillance system. Health facility data collecting system does not include information on site, type and severity of the injury. Systematic sampling of injury related visits and its circumstance is representative of total injured population46. However details regarding the circumstances surrounding different injuries must be known to those who develop preventive programs. The first step of Uganda towards establishment of injury surveillance system was to initiate hospital based trauma registry that generates relevant and timely data on causes, severity, morbidity, mortality and out comes of the injuries34. It is also shown that it is possible and useful in our country30. This will be one of the key areas that need to be further explored and encouraged because hospital records provide a useful tool for monitoring injury preventive activities in developing countries47. The surveyed health facilities do not collect information on the type of road users (pedestrians, passengers or drivers). This type of information is available only at traffic police departments and, most of the time, it is very difficult to trace and link with that from health facilities. The current data collection system does not allow for a description of injury burden in Addis Ababa. Forty four percent (N=17,764) of ‘other accidental’ causes is too big a number to lump together as “others”. It is difficult to imagine what was left out that would amount to all those cases. Furthers review is recommended to look into the specific causes of injuries packed in this category. Recommendations
Acknowledgement Special thanks go to all health facilities involved in data collection. Tireless support of senior management staffs from Addis Ababa Health Bureau, Mr. Samson Tekeste and Mr. Retta Tamene, is very much appreciated. Mr. Geremew Taye and Mr. Dagim Kassim have made very useful support during data compiling process. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08025f2.jpg] [js08025t2.jpg] [js08025f3.jpg] [js08025f1.jpg] [js08025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}