 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
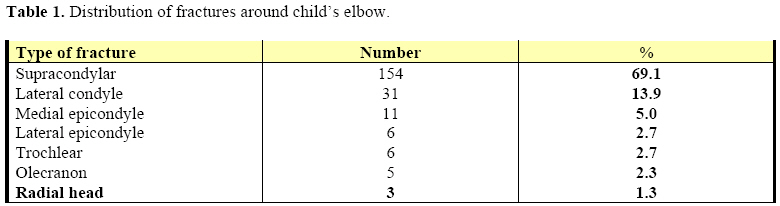
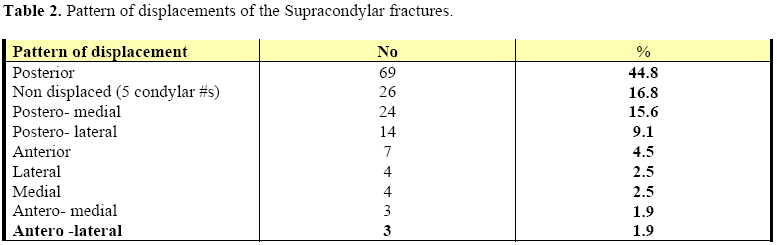
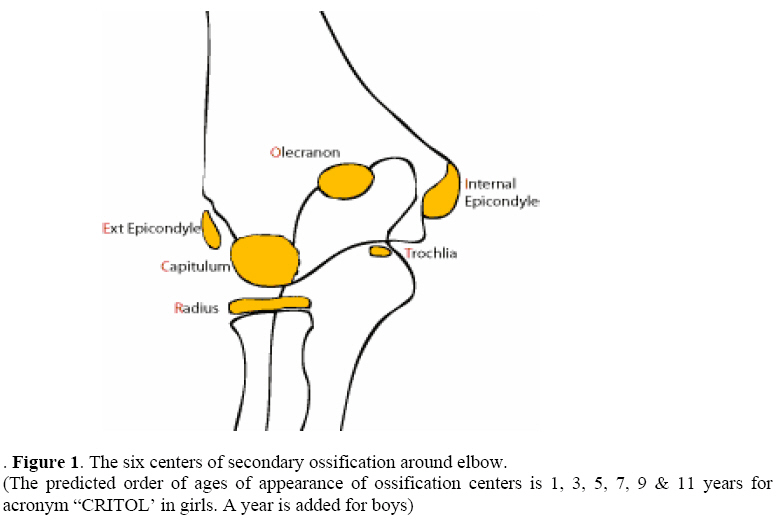
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 23-28 Fractures around child’s elbow-Radiological patterns L.W. Biruk1, D Admassie2, A. Banchiamlak3 1Assistant. Professor of Orthopedic Surgery, Addis Ababa University, Medical Faculty (AAU-MF) Orthopedic department, Ethiopia. Code Number: js08026 Background: This was a one-year prospective study aimed at evaluating the clinical and radiological patterns of the paediatric elbow fractures and determining the magnitude of the problem. The clinical and radiological pitfalls in managing such fractures were also studied and addressed. The setting was in Addis Ababa University, Medical Faculty, Department of Radiology, Tikur-Anbessa Referral/teaching Hospital. Introduction Fractures around child’s elbow are very common, accounting for about 10% of all childhood fractures. Due to the unique nature of pediatric elbows, occasionally diagnosis is difficult and some injuries are often missed unless careful radiological assessment is made. Added to this, inaccurate history, issue of child abuse and poor diagnostic facilities in our region will obscure the diagnosis. In three major studies reviewing large no of fractures sustained by children, the upper extremely accounted for 65-75% of all fractures, the most common area involved being the distal forearm. In these studies, the incidence of fractures about the elbow was consistently ranging from 7-9% of all childhood fractures1,2,3. Presence of secondary ossification centers, fragmentations seen in these centers and variability in the growing cartilage are also additional factors making diagnosis of injured pediatric elbow uneasy task. The appearance of six secondary ossification centers at the pediatric elbow is relatively predictable for age and sex, with a common acronym ‘CRITOL’4. In a combined series of 5,228 fractures of the distal humerus, 79.8% involved the supracondylar area, 16.9% involved the lateral condyle and 12.5% represented avulsion of the medial epicondyle. Both the condylar fracture & the fractures of the medial condyle had an incidence of < 1% (5,6,7,8, (12,14,4,3,15.). Elbow injuries are much more common in the skeletally immature than in older people. The peak age for fractures in distal humerus is in the 1st decade of life with most of the injuries occurring between ages 5-10 yrs. Elbow injuries are more common in boys. The study in the northern hemisphere, there is a seasonal factor with seasonal peak during the summer (while they are playing in summer vacation) and the low point during winter. The peak incidence of physeal (epiphyseal plate) injuries in most parts of the body is towards the end of skeletal maturity. However the peak age for injuries to the distal humeral physes was 4 to 5 yrs of age in girls and 5-8 yrs in boys. In most physeal injuries, the high incidence with advanced age is said to be due to weakening of the perichondral ring as it matures. Thus some different biomechanical forces and conditions must exist about the elbow to make the physis more vulnerable to injuries at an earlier age. Fracture-separations of the distal humeral epiphysis in the present series and those reported in the literature were all either type I or Type II injuries, as defined by the Salter-Harris classification. Bright et. al showed that the epiphysis is more likely to fail with rotatory shear forces than it is with pure bending forces. In the younger child, forces applied to the elbow are more likely to be rotatory shear, such as those applied in child-abuse or birth trauma; this possibly explains the higher incidence of epiphyseal separations in this age group. In the older child the forces are more likely to be the result of hyperextension of the elbow. This concentrates the force generated by the Olecranon in the supracondylar area of the humerus, resulting in supracondylar fracture 9,10,11,12,13 . Elbow dislocation is also common in elbow trauma in children. The Postero-medial dislocation, said to be characteristics with a fracture is rare. Translocation of proximal radio-ulnar is rare however the unexpected anatomic relationship is easily over looked and delayed reduction will result in permanent impairment of elbow motility. In addition to the method of radiological assessment of the elbow joint fracture by using the centers of secondary ossification age, as mentioned above, the fat pad sign is also helpful in radiological diagnosis of elbow joint fractures. There are three areas where the fat accumulation around the elbow joint area. Olecranon (posterior) fat pad sign occurs when there is occult intra articular fracture, a spontaneously reduced dislocation or even an infection14. The anterior fat pad and the supinator fat pad signs aren’t reliable. Corbett15, in his review of elbow injuries indicated that if a displacement of the posterior fat pad existed, a fracture was almost always present. Displacement of anterior of pad alone however could occur without a fracture. When reading pediatric elbow plain x-ray films it is wise to follow a certain routine pattern and a very doubtful and challenging clinical scenarios, MRI is a diagnostic option20. Methods Over a one year period, 2005-06, a total of 223 elbows in all children aged < 16 years, with injury and fracture were included/followed by the study (72 elbows with out fracture on x-rays were excluded). After proper history extraction from the child, parents or attendants, meticulous physical examination was done by an orthopedist. PA and lateral plain radiographs were taken and read by radiologist. In doubtful conditions, discussions were made among the researchers. More plain-film views & contra lateral x-rays were taken and interpreted. All the findings were recorded using a format prepared. Results Among the 223 included children, 168 (75.3%) were males and a quarter 55(24.7%) were females. The ages ranged from 1 day (two birth fractures) to 16 years, with a mode of 7.8 years. More than three fourth of the fractures happened at 5-10 years of age. Falling accidents accounted for 96% (214) of the fractures. In the majority, 66% (147), left elbow was injured. Road traffic accidents accounted only for 7 (3.1%) of the fractures and these all were boys. Two fractures were caused by a clearly evident parental abuse (bitterly beaten with sick). The most frequent type of fracture was supracondylar 69.1(154/223), followed by lateral condylar fractures in 31 (13.9%) and medial Epicondylar fracture in 11 (5%) (Table 1). No radial neck or isolated medial humeral condyle fractures encountered. Posterior fat pad sign was Positive in 171 (77%) elbows, Negative in 45 (20%) and difficult to decide in 7 elbows. Out of the 154 supra condylar fractures, 114 (74%) were in males giving a male to female sex ratio of 3 to 1. Isolated elbow dislocation occurred in one child and there was one Monteggia’s-equivalent. There were four elbows with combined/mixed injury. In 22‘difficult’ elbows radiological and orthopedic diagnoses were different, hence joint discussions and contra lateral x-rays were necessary. Diagnosis was totally missed by both groups in four patients and it was retrospectively made during follow- ups. This included: One Incarcerated medial epicondyle, Two cubitus varus and a stiff elbow with callus around Capitullar region. All of them needed further treatment that is difficult/ with poor outcome (Table 3). No MRI images were obtained due to financial constraints. Most of the displacements in supracondylar fractures were moderate or severe in 83.0% and the commonest displacement was posterior in 69 (44.8%). Postero-medial displacement was seen in 24 (15.6 %) and posterior-lateral in 14 (9.1%). There were five undisplaced condylar fractures and we grouped them in the category of undisplaced supracondylar fractures since we did not operated on them. Non-displaced Supracondylar fractures were 26 (16.8% ) (Table 2). The peak age distribution of specific fracture is shown on Table 4. Discussion In our study group of 223 elbows, fractures were found in 75.3% and 24.7% boys and girls respectively with a male to female sex ratio of 3:1 This compares with findings in other studies done by Fahey in Chicago (M:F =2:1) and a study in Hong (M:F = 2.7:1) 4,6,16,17. African boys tend to be more involved in ‘violent’ playing and sport activities than girls and hence the higher risk of traumatic injuries. The age pattern of the fractures is consistent with most reported age distribution reported in literature21. Falls were found to be the major cause of fracture of elbow joint in this study accounting for 95.9% of cases which contrasted significantly with the 3.1% due to road traffic accidents. This is similar to finding in the East African study reported in 1994. The left side elbow was more frequently affected than the right 65.9% (147) and 34.1 %( 76) respectively with a ration of l.8: 1. This is similar to that of the study in St Francis hospital6,8. The explanation may be the fact that the right upper extremity, which is the dominant one in the majority, usually protects itself from falls and is busy in some activities but the left upper limb usually simply hangs down being prone to injuries. The most frequent type of fracture was supracondylar in 69.1 % which is almost similar result to the elbow fractures in children of Denmark16 55% and in the study in St. Francis hospital6 of 60%. Major orthopedic reference books3,17,18 mention the incidence to be as high as 79.8%. The next common type was medial condylar (capitellar) fracture accounting13.9%, which is again similar to findings in those studies mentioned above. Out of 154 supracondylar fractures 74% were males. Most supracondylar fracture occurred in males (74%) and in the 5-10yrs age group (75%). The peak age was 7 years which is consistent with many other studies. Elbow injuries are much more common in the skeletally immature than in older people including physeal unlike fractures in most parts of the body is toward the end of skeletal maturity. This study also showed this truth that most of the fractures are between the ages of 5-10yrs 3,4,6. Capitallar fracture accounted for 13.9% with 71% of them occurring in the 5-10yrs aged children. Trochlear fracture was slightly commoner and for this we found no apparent explanation. The supracondylar fracture was associated with some displacement in 83% of cases of which posterior displacement accounted for 44.8% and posteromedial in 15.6% and posterolateral in 9.1%. Other rare types of displacements were anterior, anteromedial, lateral and medial all in 3.7%. The non-displaced supracondylar fracture accounted for only 16.8% of cases. Similar findings have bee reported in many previous studies1,2,3,6,7,11,12,13. Posterior fat pad sign is one of the important radiological signs to diagnosis fracture of elbow joint in children. In this study positive posterior fat pad sign was recorded in 76.7% of cases, was negative in 20.2% and inconclusive in only 3.1%. This correlates well with findings in other studies that had a positive fat pad sign of 87% and negative result of 13%. The slightly higher negative fat pad sign seen in our study could be explained by the fact that the children had very gross soft tissue swelling from massage by bone setters before coming to Hospitals. Recommendations We recommend the following:
Acknowledgments To the AAU Radiology Department for letting us conduct and publish the research findings and to the members of SSE for suggestions and comments forwarded during the presentation at Hilton Addis. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08026t2.jpg] [js08026t4.jpg] [js08026f1.jpg] [js08026t1.jpg] [js08026t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}