 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
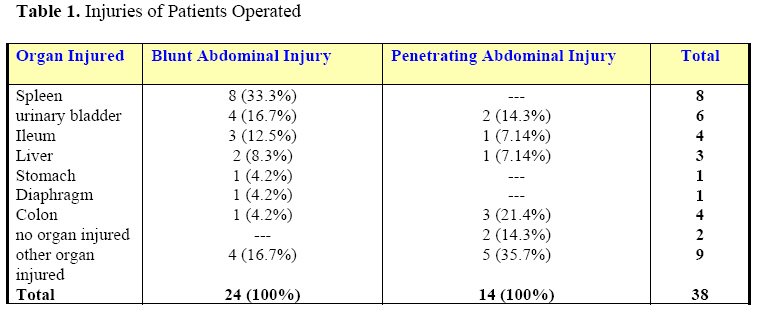
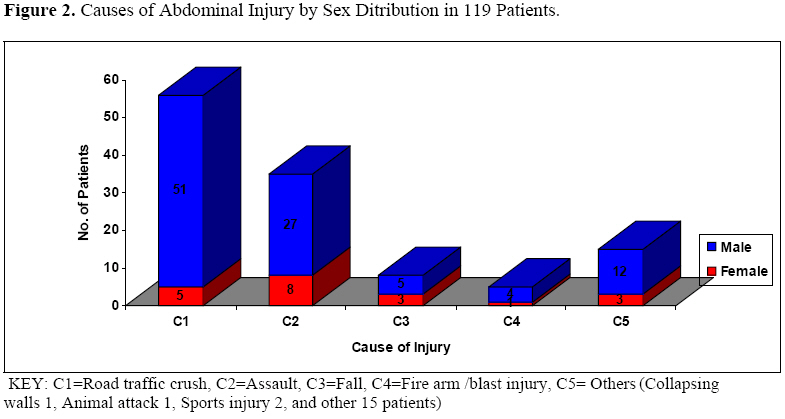
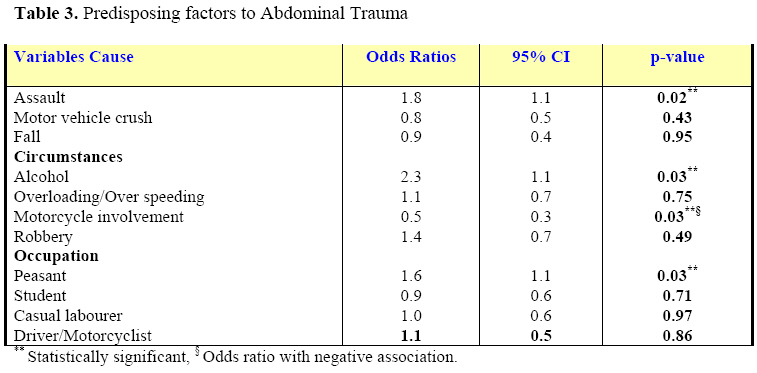
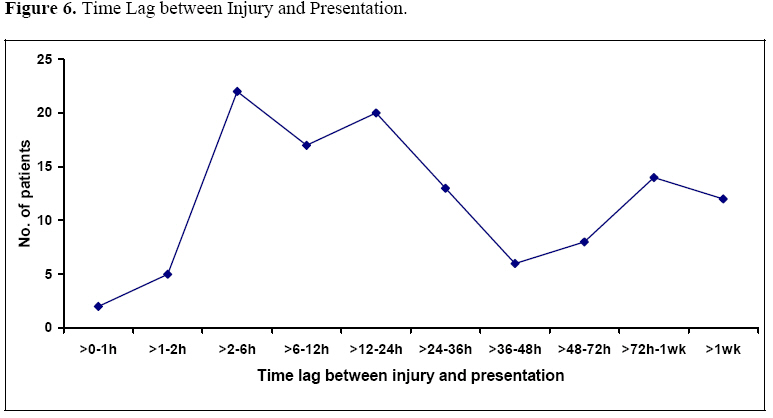
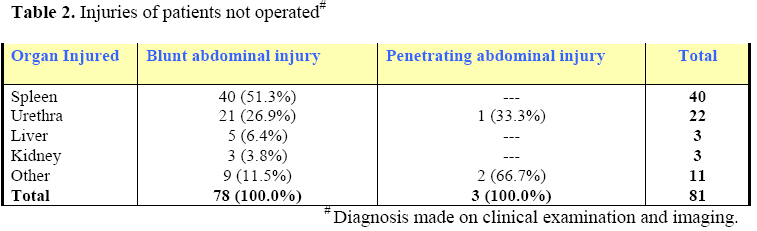
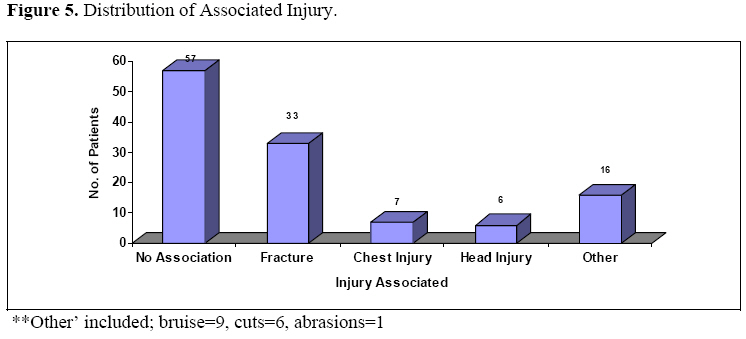
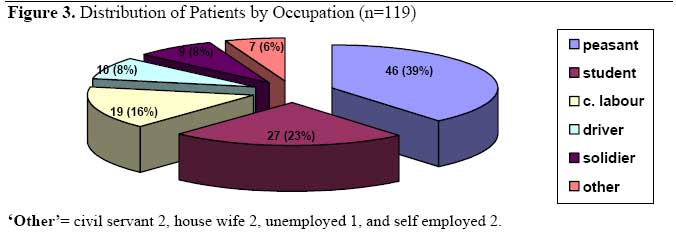
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 29-36 Abdominal Injury at Mbarara Regional Referral Hospital, Uganda G. Ruhinda1, P. Kyamanywa1, D. Kitya1, F. Bajunirwe2 1Department of Surgery, 2Department of Community Health, Mbarara University of Science and Technology, Mbarara, Uganda . Code Number: js08027 Background: Trauma poses a major public health challenge in Africa. This study was aimed at determining the prevalence, patterns and predisposing factors of abdominal injury in Mbarara Regional Referral Hospital (MRRH). Introduction Injury accounts for 10% of all global deaths, according to world health organization (WHO) study on global burden of disease 1990.2,3 For all age and sex groups, injuries are a major cause of emergency department visits.4 Abdominal trauma is a leading cause of morbidity and mortality among all age groups1. While it has been stated that, motor vehicle crushes are the commonest cause of abdominal injuries5. there is insufficient data that has been published on abdominal trauma in Uganda6. Mechanisms of injury often determine the severity of abdominal injury and the likely associated injuries. The associated injuries may divert the physician's attention from potentially life-threatening intra-abdominal pathology7. Accurate and timely recognition can be difficult, and delay in diagnosis is associated with significant morbidity and mortality8. Patients and Methods A non-interventional, cross sectional study, of patients admitted with abdominal trauma to the department of surgery of Mbarara Regional Referral Hospital between 1st of August 2005 to 31st of March 2006 was undertaken. Mbarara Regional Referral Hospital (MRRH) is a government-owned referral and teaching Hospital. The Hospital is situated along the Kampala-Kabale highway. MRRH has an annual enrolment of 17,400 in-patients and 63,300 outpatients. The average in-patient annual enrolment for surgical wards is 2,497 (15%). An interviewer-administered pre-coded questionnaire was used for data collection. Where necessary, a review of patient’s medical records (i.e. referral form, if he had been referred) was done. For the patients that underwent surgery for the injuries, details of the operation findings were obtained from the operation notes and through liaison with the surgical team. Results A total of 836 trauma patients were admitted during the study period of whom 119 (14.2%) patients had abdominal injury, and these made the study population. Seventy seven of the 119 (65%) were found to be non-intentional while 42(35%) were intentional injuries. The ages ranged from 3 to 88 years with a median of 27 and a mean of 30.3 years There was a predominance (83.2%) of males, only 16.8% were females; giving a male to female ratio of 5:1. Children under 12 years were only 10 (8.4%) with a male to female ratio=1:1. Fifty two percent of the injuries were sustained on the road with 30.2% occurring on village road, 13.4% on high way and 9.2% on urban road. Injuries sustained at home accounted for 15%, work place 13%, garden 6%, recreational places 8% and others 6%. Most home injuries were assaults (50.0%) followed by falls (22.2%). The spleen was the most commonly injured organ among the patients that had exploratory laparotomy while the liver was the least injured (Table 1). Mechanism and Diagnosis by injured organ Blunt Abdominal injury accounted for 85.7% [95% CI=78.1%-91.5%] and penetrating abdominal injury for 14.3% [95% CI=8.5-21.9%]. The majority (70.6%), of penetrating abdominal injury resulted from stub injuries and 29.4% from fire arms. Four (40%) children under 12 years were operated, one was a negative laparotomy. Abdominal injury in 52% was more prevalent among patients injured in motor vehicle crushes (than any other cause of injury (p-value =0.17). Other injuries followed closely (Figure 2). Table 3 shows the factors considered to have contributed to occurrence of the trauma.The risk factors for abdominal injury included assault, use of alcohol, use of motorcycle as a means of transport and being a peasant. Sixty five percent of patients arrived to hospital in private cars; only 17% used formal ambulances, 3% used police vehicles, 12% arrived on motorcycles and the rest either on foot or other improvised mode of transport. The majority of patients presented more than six hours after the injury, as shown in Figure 6. Discussion Trauma, in all its varieties continues to pose a major public health challenge. This study has shown the prevalence of abdominal injury and uncovered important findings in patterns and predisposing factors in patients admitted to Mbarara Regional Referral Hospital. Social demography of abdominal injuries It is well known from other studies in the region, that there is a male predominance in injuries11. In this study, the male to female ratio was 5:1, lower than reported in other hospital based studies in Africa11,12,13. Males are the bread earners of most households, and are probably more involved in activities that predispose them to injury in the process of trying to earn a living. The mean and mode ages were 30.4 years and 27 years respectively. This represents the economically productive age group. Peasants formed 29.9% in this study followed by students (24.4%) which was was consistent well with findings by Smith et al13. As one would expect, at the two extremes of life, the rates of abdominal injuries were low. The study also showed that violence against females in the home is still rampant in our communities. Prevalence of abdominal injury Abdominal injuries in this study had a prevalence of 14.2% (CI=12.0% to 16.8%). In comparison with other injuries like fractures, with the highest prevalence at 29.2% (CI=21.0% to 38.5%) as shown in Figure 5. Prevalence of 14.3% for penetrating abdominal injury in this study compares well other studies from Africa. Musau et al10 in Kenya found stab wounds to account for 64.2% of penetrating injuries, which is a similar result to the 64.3% recorded in this study. A study from from Nigeria14 showed a higher prevalence of penetrating abdominal injury secondary to gun shot wounds as compared to the 29.4% found in this study. The prevalence of blunt abdominal trauma in this study was 85.7% which is much higher than the corresponding figure of 46.3% found by Edino14 in Nigeria. The fact that Mbarara is located on the on a major highway may explain the high number of blunt abdominal injuries recorded in our series. In this study, 52.0% of injuries were sustained on the road which was in agreement with other studies which have shown that motor vehicle crushes are the biggest cause of blunt abdominal injury16,17. While there is a general consensus that, the spleen is the most commonly injured organ in blunt abdominal injury, no such agreement exists in penetrating injury14,16,19. Cause and Circumstances of the injury: Abdominal injury is more prevalent (52.0%) among patients injured in motor vehicle crushes (Figure 2) than any other cause of injury (p-value=0.17). Other injuries follow closely (Figure 2). Similar studies on injuries in this hospital and from other areas show a similar trend.14,20,21 Road transport (cars, bicycles, motorcycles) is the commonest form of transport in Uganda, thus most injuries occur on the road (p-value=0.04).6 Village roads accounted for 30.25%, while high way and urban roads account for fewer (Figure 3). Similar findings have been observed by other researchers.14,16,25 It is possible that vehicles in the more rural areas are in poor mechanical condition and are driven by learners and unlicensed drivers/riders on the village roads, since it is contrasted sharply by a low accident rate (9.24%) on the urban roads (Figure 3). Further more, there is no effective policing on the roads in the more rural areas. It has been shown that, there is significant association between blood alcohol levels and road traffic accidents22. Our study confirmed that there is a significant association between abdominal trauma and alcohol drinking as a predisposing factor in abdominal injury (OR=2.32, CI=1.14 - 4.74). This odds ratio shows an increased risk to abdominal injury in people who took alcohol (p-value=0.03) as shown in Table 3. A significant number of accidents (9.2%) happened in association with a motorcycle taxi known as bodaboda in Uganda, (p-value=0.03). However, it causes fewer abdominal injuries than those on the other parts of the body as has been observed by other researchers.21 Assault accounted for 29.4% of the abdominal injuries. Half occurred at home, the rest at the work place [OR=2.02 (95% CI=1.05 - 3.89), p-value=0.03] and the victims were more likely to be women, and this is echoed by other studies23,24 . The reasons advanced were mostly domestic violence and punishments being administered to students, factory and farm workers. Patterns of Abdominal injury Eighty one patients (68.1%) were not operated, this has become popular in some areas26. In the non-operated group, the spleen injured in 51.3%, was the top organ involved. Further more, a strong association was observed between urethral injury 21 (26.9%) and pelvic fracture, where 30% of pelvic fractures were associated with urethral injury. The liver and kidney accounted for the rest (6.4% and 3.8% respectively). Interestingly there was only 1 (33.3%) urethral injury and only 2 patients with minor injuries in the non-operated group. The spleen was the most commonly injured organ (7.8%) in patients with blunt abdominal injury who had surgery. Ruptures accounted for 36.8% of the injured spleens in patients who were operated, followed by lacerations 14 (28.9%). The urinary bladder accounted for 3.9% and all were ruptures seen at operation. The rest were ileum and liver ruptures. The colon injured in 17.6% was the commonest organ involved in penetrating trauma followed by the urinary bladder in11.8%. The liver and ileum were damaged in only 2.9% each. Two patients with penetrating abdominal injury were found to have normal findings at laparotomy. This differs from studies reviewed, whose analysis combined both blunt and penetrating trauma.14,15 This could be because interpersonal violence with stub and gun shots is very prevalent in the geographical area where he carried out the study. Although we did not specifically examine missed injuries, it is recognized that this may be a concern in non operated patients. In this study, a patient with penetrating abdominal injury was more likely to be operated upon. Penetrating injury was found to be less associated with other injuries (52.9%) than blunt injury (47.1%)27. Head injuries were the second commonest association, and not the first, as was observed by Landau et al., in Cape Town27. It is possible that in Mbarara town, with no pre-hospital care and ambulance system, not as many severely head injured patients would reach hospital as it would be in Cape Town, South Africa. The patterns of injury in children were similar to the adults. Only four children were operated and one was a negative laparotomy. None of the children is known to have died. Observations by some researchers do not correlate well with this current study especially on causes which were different20,33 . MVAs caused fewer injuries (30%) which could be due to the small sample size that was captured. This was so because we not specifically look at abdominal injuries in children but in the general population, thus numbers are not easily comparable. Pre-hospital care There was a bimodal presentation of patients to hospital at 2-6 hours and 72 hours to one week (Figure 6). This was in sharp contrast with another study in Uganda which found that two-thirds of patients in Kampala arrive in hospital within thirty minutes29. This is possible since our study was conducted in an area where patients come form semi urban and rural areas where transport means form such areas is difficult to get, and there is no system in place (e.g. ambulance services) to bring the injured to hospital in time. The second peak represents patients that were referred from other health units. In studies reviewed (from UK and Australia), trauma patients reach a competent trauma centre in the shortest time possible, usually less than one hour31,32. Most patients (65%) arrived at the hospital by public or private means of transport, some by the police ‘pick-up’ vehicle, and few referrals by ambulance. The delay in presentation to hospital, and the mode by which patients arrive, shows gaps in the referral system and is clear testimony that pre-hospital care is lacking. Conclusions The common pattern of abdominal injury was blunt abdominal injury (85.7%) with prevalence of 14.23%. Young adults are the most affected, and MVAs cause the highest number of abdominal injuries. The major predisposing factors are assault and alcohol consumption. The hallmark of trauma management is prevention, thus initiatives to minimize trauma must be geared towards it. This requires public education and enforced legislation. Injury control centre-Uganda in conjunction with the Uganda police in 2004 organized campaigns on road safety, but these need to be continued to see a valuable outcome. Acknowledgements Thanks to the Government of the Kingdom of Belgium (and BTC – Uganda), for the financial support, members of staff in the Department of Surgery – MUST and to Dr. R. Twesigye for helping with the statistics. . References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08027t2.jpg] [js08027f6.jpg] [js08027f3.jpg] [js08027f5.jpg] [js08027t3.jpg] [js08027t1.jpg] [js08027f2.jpg] [js08027f4.jpg] [js08027f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}