 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
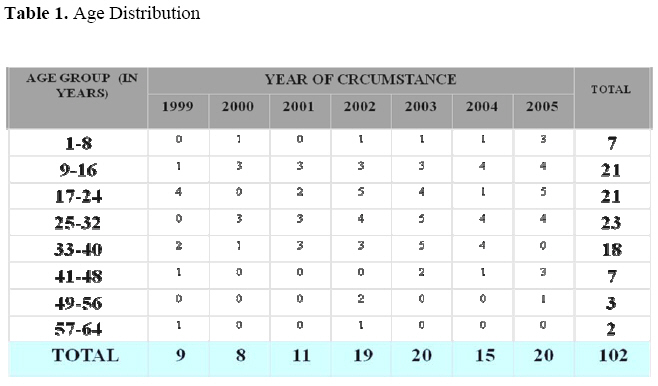
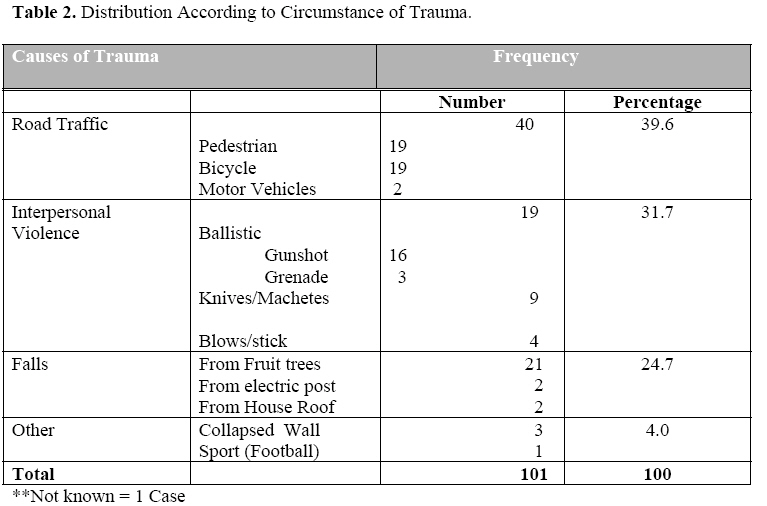
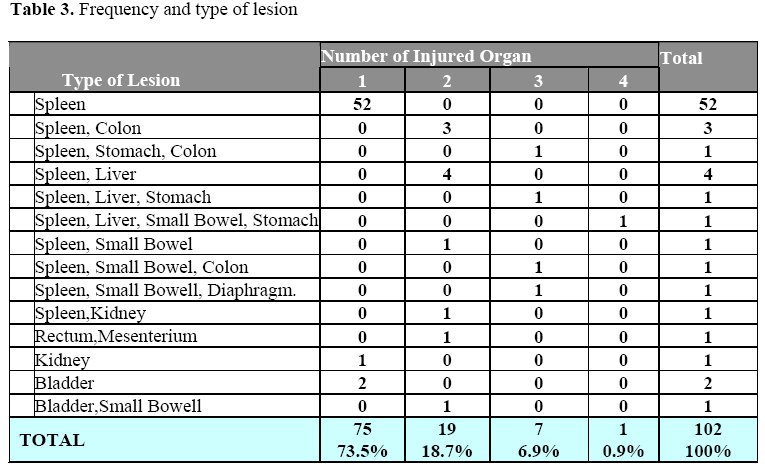
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 37-42 Traumatic Haemoperitoneum at Butare University Teaching Hospital M. Makanga, F. Mudekuza, M. Ndayishyigikiye, I. Kakande Surgical department, CHUB, National University of Rwanda Code Number: js08028 Background: An epidemiological study on the traumatic haemoperitoneum cases that underwent surgery over a 7 years period from January 1999 to December 2005 was carried out in the Surgical Department of Butare University Hospital, Rwanda. The main aim of our study was to determine the epidemiological character, development and management of posttraumatic haemoperitoneum. Introduction In our African settings, traumatic haemoperitoneum (presence of blood in the abdominal cavity) has a particular emergency character of life threatening which can be fatal for the patient, if not diagnosed early, managed properly and in time. Abdominal trauma can occur isolated or as a component of polytrauma. The prognosis of the patient depends on many factors that included the pre-morbid pathological condition of the patient, the cause and nature of the trauma (e.g. road traffic crush, assault or gunshot injury), the type of organ lesion, the associated intra-abdominal lesions, the quantity of blood in the abdominal cavity and the condition and rapidity in management and patient care. The intra abdominal lesion can be due to a closed trauma (85%) or an open trauma (15%). In our African settings, the delay of referral, diagnosis and often in the context of polytrauma, with post traumatic haemoperitoneum can have a particular emergency character of life threatening which can be fatal for the patient, if not diagnosed early, managed properly and in time. This study was aimed at determining the causes, presentation, operative findings and outcome of management of traumatic haemoperitoneum. Patients and Methods This was retrospective descriptive study, including 102 patients operated for posttraumatic haemoperitoneum. Data was collected from patients’ clinical files and operation register. Information obtained was recorded on a pre-established questionnaire. Data obtained was were analyzed using Epi Data and SPSS computer programs. Results Over a 7 years period between January 1999 and December 2005, a total of 2114 patients were operated for abdominal conditions of whom 102 (4.8%) had surgery for posttraumatic haemoperitoneum. The number of cases ranged between 8 and 20 cases annually. There was a preponderance of males both in children and adults with a male to female sex ratio of 5: 1. The M: F sex ratio in children was 4.4: 1 (22: 5) (4.4: 1) and in adults, 63 were males and 12 females (M:F Ratio = 5.25: 1). Table 1 shows the age distribution. The age varied between 5and 62 years with the average of 25.7 years The 25 to 32 years age group was the most affected. Seven patients were children under the age of 8 years. Only 12 (11.8%) of patients were aged above 48 years. The 9 – 32 years age group accounted for 65 (63.7%) of cases. Peasant farmers and students contributed 32.45 and 27.5% respectively. Road traffic accident was the most frequent cause, leading to 40.2% cases of haemoperitoneum (Table 2). The majority (71.6%) of cases reported for treatment within the first 6 hours after trauma and 84.3% were seen within 24 hours after sustaining injury. Only 36 (35.3%) had been referrals from district hospitals. The rest came on their own. Clinical features were mainly those of shock and pallor. The abdominal findings included abdominal distension, tenderness, rebound tenderness and guarding, rigidity and shifting dullness. To confirm suspicion of haemoperitoneum, abdominal paracentesis and diagnostic peritoneal lavage were performed in 48 cases and were all positive for blood. Half (50.9%) of the patients had a haemoglobin level of less than 10g/dl. The management consisted of resuscitation, laparotomy plus specific surgical procedure for the injured organ(s) and transfusion or autotransfusion depending on the type of lesions found. The estimated quantity of blood loss varied between under 500cc in 30 cases, 500cc to 1000cc in 31 cases and more than 1000cc in 41 cases mainly those with spleen rupture. Most (73.5%) of the patients had one organ injured (Table 3). In 52 (51.0%) of the cases, the spleen was injured. Splenectomy was done in 44 and splenorrhaphy in 7 cases. Associated extra abdominal lesions were presented in 38.2% and mainly involved the skull (15 cases) and limbs fractures (14 cases). The length of hospital stay varied from 14 hours to 134 days with the average of 17.55 days. The long stay in hospital for few patients was due to associated pathological conditions such as polytrauma, extra-abdominal lesions. The outcome of management was good in 82 (80.4%) and 12 (11.8%) had some postoperative complications such as wound sepsis. There were 8 deaths, a 7.8% hospital mortality. Discussion Our study has shown that when presented with a patient with traumatic haemoperitoneum, the organ most likely to have been injured is the spleen mostly following road traffic trauma. The hospital incidence of haemoperitoneum in our study was similar to that reported by Pierre1. Like in other studies the young males in their most productive age are mostly involved2,3,4,5. Our findings are in agreement with what others have found that road traffic accidents were the main cause of abdominal injuries6,7,8 followed by interpersonal violence as the second cause1,8,9. The average time interval between trauma and arrival to hospital emergency unit in our study was a little bit longer than what was reported from other developing countries2,10. Our findings confirmed what many authors 1,2,10,11,12 have found that diagnostic peritoneal lavage or the abdominal paracentesis with the needle is the easiest way to diagnose the hemoperitoneum. The spleen rupture was the main organ leading to an significant hemoperitoneum2,6,11,13,14. Most splenectomies done were due to spleen rupture stage III and IV on patients with underlying splenomegalies, which is similar to what has been reported from other developing countries1,2,5,11, Some authors advised other alternatives: abstention, monitoring, splenorraphy in case of spleen rupture stage 1 and 215,16. Auto transfusion, admitted by many authors15,16,17 when respecting correctly the rules of its use, and in case of spleen rupture alone, without associated injury, seems to be a good indication to give the patient his own blood, avoiding the risk of HIV and/or hepatitis infections. According to many authors, the post operative outcome was satisfactory; death rate, unfortunately high, is due to the delay on arrival to the emergency, polytrauma and associated extra abdominal lesions2,4,9. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08028t1.jpg] [js08028t4.jpg] [js08028t5.jpg] [js08028t2.jpg] [js08028t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}