 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 43-51 The Effects of Dual Micronutrient Supplementation on Thyroid Function in School Children: An Experimental Study C. Abuye1, Y. Berhane2, Z. Getahun1, G. Akalu1, T. Ersumo3 1Food Science and Nutrition Research Department, Ethiopian Health and Nutrition Research Institute, Code Number: js08029 Background : The presence of iron and or vitamin A deficiency in children limits the effectiveness of the iodine intervention program in areas where iodine deficiency is endemic. This study was aimed at assessing the role of dual micronutrient supplementation on thyroid function in severe iodine deficient school children age 6-16 years in Ethiopia. Introduction Micronutrient deficiencies affect millions of people around the world particularly in developing countries1,2. Iodine deficiency is a world wide health problem especially in developing countries affecting about 800 million people in Asia, Africa and South America. Iodine deficiency Disorders (IDD) are the leading cause of mental and physical retardation in iodine deficient areas of the world3,4. It has been reported that vitamin A deficiency (VAD) is the most common cause of blindness and increased morbidity and mortality in children; it causes night blindness in pregnant women in many developing countries1,5. Iron deficiency anemia affects 40% to 60% of young children globally and is categorized by WHO as one of the top ten serious health problems in the world6. Iron deficiency Anemia adversely affects such vulnerable groups as pregnant and lactating women and children in a number of ways in most developing countries7. The coexistence of micronutrients (iodine, iron and vitamin A) malnutrition sharing common functional ground in health consequences has been reported5,8. Iron deficiency anemia adversely affects thyroid metabolism of iodine and may reduce the efficacy of iodine prophylaxis in goiter prevalent areas. Iron deficiency reduces plasma thyroxine and triiodothyronine concentration and may elevate production of thyrotropin. Experimental study on Iron supplementation in goitrous iron deficient children improves their response to oral iodized oil in treating goiter9. In animal study, VAD decreased thyroidal iodine uptake and impaired thyroglobulin (Tg) synthesis thereby increasing thyroid volume10,11. A study conducted in Morocco showed that VAD, in children with severe IDD increased TSH stimulation and thyroid size, the authors concluded that concurrent iodized salt and vitamin A supplementation to IDD and vitamin A deficient children improves iodine efficacy12. Previous studies in Ethiopia13 however showed no functional relationship between iodized oil and vitamin A and iodized oil and iron supplementation. Iodine, Iron and vitamin A deficiencies are common and coexist in many parts of Ethiopia at an endemic scale14-19. National surveys conducted in Ethiopia in 2005 20,21,22 revealed 39.9% TGR in children, 35.8% TGR in child bearing age women and 1.7% Bitot spot in children while iron deficiency anemia was 54% in the under five children and 27% in child bearing age (15-59 years) women23. To control and eradicate the problem of micronutrient malnutrition, strategies such as dual, iodine and iron24,25 or triple, vitamin A, iron and iodine26 supplementation are under investigation. Study results released so far on relationship of micronutrients efficacy are mixed5,813,26,27. This study was undertaken in school children affected by multiple micronutrient deficiency problems to assess the efficacy level of dual micronutrient supplementation on thyroid function. Materials and Methods From 2006 to 2007, an experimental study was designed to assess the efficacy of combined micronutrient supplementation on thyroid physiology. The combinations were oral iodized oil capsule + vitamin A, oral iodized oil + iron, and iodized oil alone. This study was undertaken in two elementary schools found in goitre endemic villages of Gofa district, 550 km Southwest of Addis Ababa, the capital of Ethiopia. The schools were three km apart from each other. The population of children in the schools was about 1900. The selection of the schools was based on high prevalence of goiter20 and vitamin A22 deficiency. All school children volunteered to participate in the study upon request. The study subjects were clinically screened for goitre, vitamin A and iron deficiency. All 397 children aged 6-16 years with visible goiter grade, of which 6.1% and 10.3% with vitamin A and iron deficiency respectively were included. Total population of the Woreda was about 250,000, more than 95% living on subsistent agricultural economy28. Maize and fruits cultivation were seasonal and mainly rain dependent. The staple diets were root crops, porridge and bread of maize. Fruits were primarily cultivated in some villages but used as means of generating cash income22. Iodated salt was not found in the area20. As summarized in flow chart 2, at the baseline attention was directed to name, addresses, age, sex, weight, height, and collection of casual urine, blood, and stool samples. Disposable syringes with needles were used to collect venous blood samples while urine was collected in iodine free test tubes. Stool analysis and de-worming with Mebendazole (Cadila, Pharmaceuticals India) was done subsequently. A week after de-worming study subjects were allocated into groups of intervention. All children with visible goitre (n=332) but without iron and vitamin A deficiency were grouped into four groups (A, B, C and D). Similarly, children with clinical sign of vitamin A deficiency (n=24) were randomly allocated into group A and B while iron deficient (Hb<11g/dl) children (n=41) were assigned into group C and D. Group A, B, C and D consisted 95, 95, 103 and 104 children respectively. The groups were administered with their respective deficiency micronutrient under close supervision of the investigator and school teachers. Group A was administered 400mg iodized oil capsule (Lioiodal Guerbet Laboratoire, France). Group B received iodized oil (400mg) + vitamin A capsule (200,000 IU as retinyl palmitate) (Accucaps Industries, Canada) and then additional dose of vitamin A was supplemented at six month. Group C was administered 400mg iodized oil capsule and group D 400mg oral iodized oil + iron (100mg ferrous sulphate with folic acid) (Medreich, Bangalore India) and then iron twice per day up to six weeks. Every child was attended while taking iron dose one in the school before the start of the class and the other at home. During iron supplementation period children were closely inspected in the school for malaria problem. Post intervention data; weight, height, casual urine samples, blood, and clinical data on goiter grade were collected subsequently at six and eleven months. Goiter grade was clinically examined using WHO recommended method 29 which include:
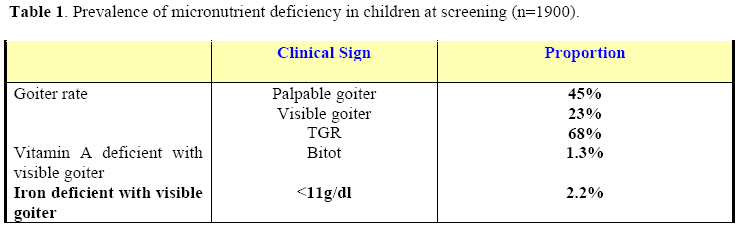
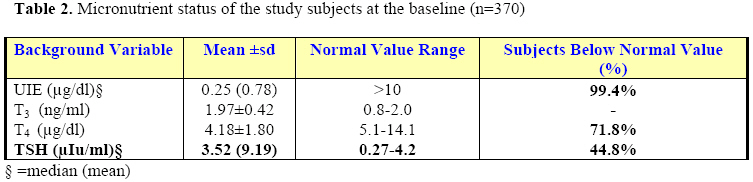
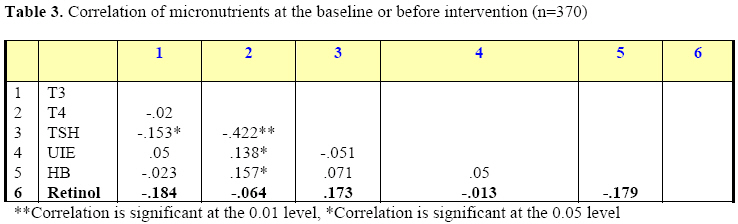
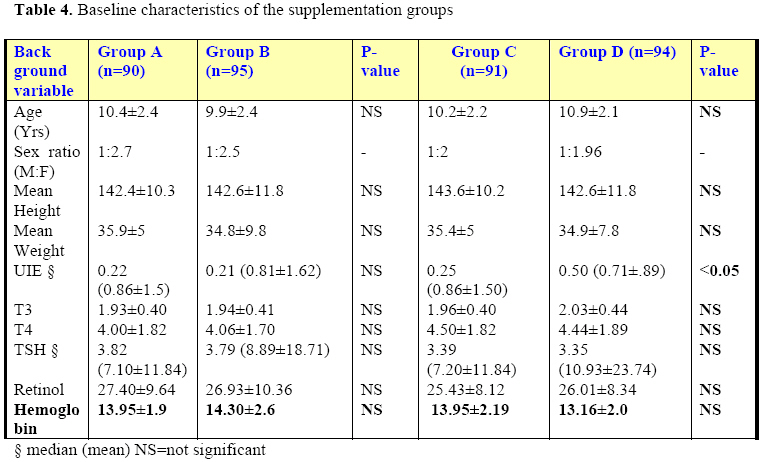
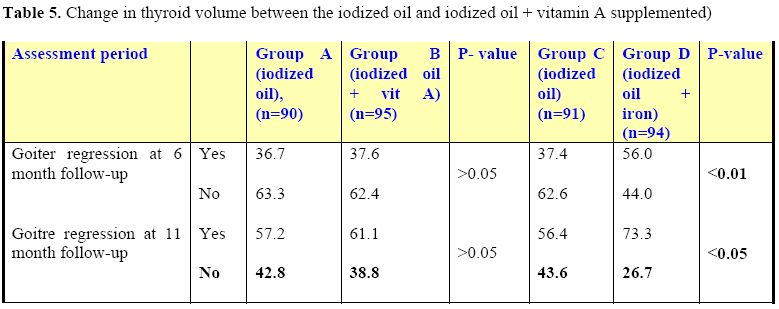
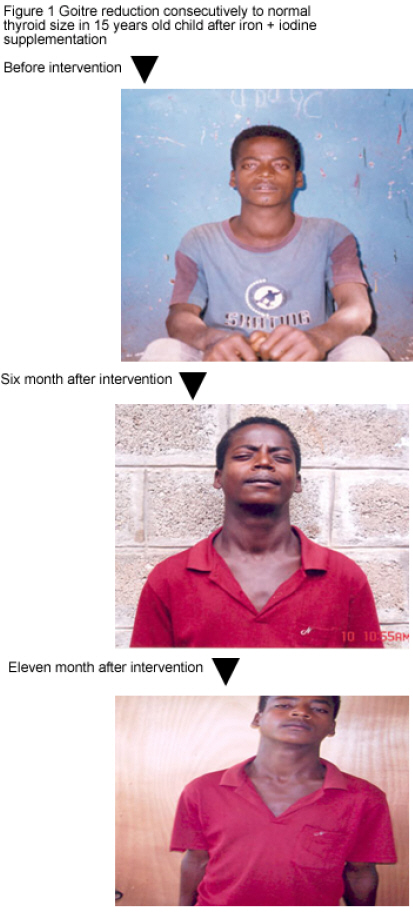
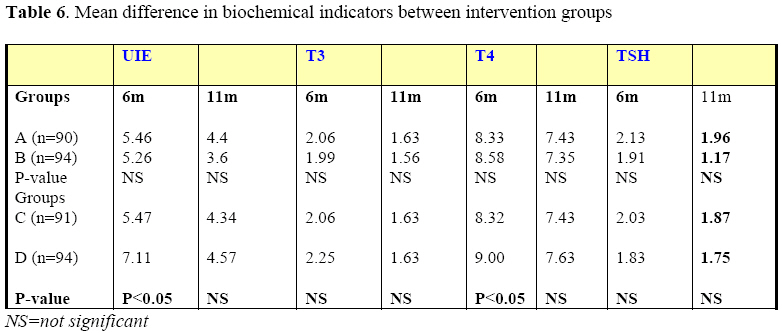
This method was convenient in the absence of ultrasound to inspect goiter/thyroid volume reduction from one category. Due to lack of resource ultrasound was not used to estimate thyroid volume. VAD sign (Bitot spot) was used to assess vitamin A status clinically at the field. Experienced senior nutritionist did the clinical examination. Besides clinical examination, photographs were used to inspect thyroid gland regression in few cases from each intervention arm. Portion of the collected venous blood samples were used to determine the hemoglobin concentration at the field using HemoCue Hb 201+ (Hemocue AB, Angelholm Sweden). The blood samples were centrifuged and serum was collected and stored in a deep freezer (-800c) until analysis. The thyroid hormones, T3 and T4, and TSH were measured at EHNRI laboratory using Elecsys 2010 (Germany, 2001). Urinary iodine analysis was done using wet digestion modified method of Sandell-Kolthoff30. Serum samples were analyzed for vitamin A (retinol) using High Performance Liquid Chromatography (HPLC) (Varian Chromatography System, USA). Initially hemoglobin and retinol were measured in all study subjects. But in post intervention period, retinol level was measured in group A and group B while hemoglobin level was determined in group C and group D. Weight to the nearest 0.1KG and height to the nearest 0.1cm were measured using weight and height scales. The previous studies31 indicated that goitre reduction three months after supplementation of iodized oil was 20% in school children. At α (one tailed) = 0.05 and probability of observing reduction (power) = 80%; β = 0.20, number of children needed to determine at least 38% reduction of goitre in double supplementation of micronutrients was calculated. Proportion of reduction (P2) in iodized oil supplemented group was 0.20. P1 (reduction in double micronutrient supplemented group) was 0.38. The smaller of the two values is 0.20, and the difference between them (P1 – P2) is 0.18. α (one tailed) = 0.05; β = 1-0.8=0.20. The required sample size for each group from the table was 109. Actual number with visible goitre grade and enrolled for intervention was 397 children of which, 6.1% and 10.3% with vitamin A and iron deficiency respectively. SPSS/PC was used for data entry and analysis. As the data was not normally distributed, difference between proportions (goiter reduction) or distribution of continuous variables between two groups was assessed using chi-square test for independence and Mann-Whitney U test respectively. A total of 370 (93%) of children (90, 95, 91, and 94, in group A, B, C and D respectively) who completed the three round follow up were included in the final analysis. The total missing subjects in any one of the follow up period due to changing school, leaving the area and unknown reason was 6.8%. Ethical clearance was obtained at two different levels; from Research and Ethical Committee at the Ethiopia Health and Nutrition Research Institute (EHNRI) and from school committees, composed of teachers and parent. All students gave informed consent and volunteered to participate in the study. Results All 1900 children present in the schools at the day of the visit were included in the clinical evaluation for goitre grade, Bitot spots and anemia (Table 1). The total goiter rate (TGR) in the school community was 68% (37% palpable and 31% visible). Vitamin A deficient subjects with bitot spots were 24 (1.3%) while iron deficient children were 41 (2.2%). Biochemical results indicating micronutrient status of the study subjects at the baseline was given by the normal value range in Table 2. According to the urinary iodine excretion levels, >90% of the study subjects were iodine deficient. Similarly on average, 71.8% of the subject had thyroxin (T4) values less than the cut-off point for normal and 44.8% had higher thyroid stimulating hormone (TSH) levels again indicating iodine deficiency. The correlation between biochemical parameters related with thyroid function was assessed before intervention (Table 3). TSH significantly (negatively) correlated with the two thyroid hormones, T3 (P<0.05) and T4 (P<0.01). Hemoglobin and UIE significantly (P<0.05) positively correlated with T4. Comparison of baseline data between groups was presented in Table 4. Baseline data on anthropometrics measurements and biochemical parameters were compared between groups. All variables between group A and B and, group C and D were not significantly different except UIE which was significantly lower (P<0.05) in group C than group D. Thyroid volume reduction was compared between groups in Table 5. In group D, thyroid volume regression was significantly higher at six (P<0.01) and eleven (P<0.05) months after intervention than in group C. Pronounced goitre reduction was observed in group A and group B but the difference was not significant (P>0.05) during the two post intervention periods. Further in-depth analysis was done in only vitamin A deficient subjects in the two groups and the goitre reduction was not again significantly different. Similarly goitre reduction was assessed between anemic group and the difference was significant and stronger (data not shown). Generally more than 50% goiter reduction was noted in all supplementation groups (A, B, C and D) at 11 month after intervention. As indicated in Figure I, sharp goiter reduction, to the level of normal thyroid volume was noted in group D (iron + iodized oil). Goitre reduction in group A and B was also noted but the difference was not quite clear by photographs Comparative biochemical results between group A and B, and group C and D were given in Table 6. At the baseline all parameters were not significantly different between intervention groups. Post intervention biochemical results between group A and group B were not significantly different. However, in group C and group D, T4 and UIE were significantly (P<0.05) higher in group D than group C. Although not significant, relatively T3 was higher and TSH was lower in group D (iron + iodized oil) than group C after intervention, The correlation between biochemical parameters related with thyroid function was assessed in the study subjects (post intervention) (data not shown). In group D hemoglobin level significantly (P<0.05) correlated with thyroid hormone T4 at eleven month after intervention. T4 significantly (P<0.01) correlated negatively with TSH, and positively with UIE (P<0.01) six month after supplementation. Similarly at eleven month after intervention, T4 significantly (P<0.01) correlated negatively with TSH, positively with UIE (P<0.01) and Hemoglobin (P<0.05) concentration. Discussion The results of this study illustrate the severity and coexistence of three micronutrients deficiencies namely vitamin A (1.3%), iodine (68.0%) and iron (2.2%) in school children. According to the WHO3,32 classification the magnitudes of both IDD and VAD problem were severe in the affected children. This study depicted that goitrous children supplemented with iron + oral iodized oil capsule had significant goitre reduction than oral iodized oil alone supplemented groups. In each intervention group, about 22% of the children with goitre were iron deficient. The mean concentrations of T4 and UIE in iron + iodine supplemented group were significantly higher than the iodine alone supplemented group at 6 months after intervention. Although not significant, TSH level was also relatively lower in iron + iodine supplemented group than iodine alone supplemented group C at the two post intervention assessment periods. Hemoglobin level at baseline in all study subjects and at eleven month after intervention in group D (iron + iodine supplemented group) significantly (P<0.05) correlated with T4. The significant goitre reduction in group D (iron + iodine supplemented) than group C (iodine alone supplemented) and the significant correlation between hemoglobin and thyroxin levels at baseline and eleven month after intervention may indicate that iron deficiency or iron supplementation has an influence on thyroid function. Reports on the efficacy of dual micronutrient supplementation/fortification on thyroid function were mixed. Inline with our findings, studies from Cote d’ Ivoire5 Morocco25 depicted that iron deficiency anemia in children limit the effectiveness of an iodine intervention program. In Cote d’ IVoire when compared with baseline, decrease in thyroid volume/goitre was not significant in anemic children than in non-anemic 30 weeks after administration of oral iodized oil. Other studies similarly indicated that iron deficiency anemia hampers thyroid function and may reduce the efficacy of iodine intervention in goitre endemic areas8,9. However, in contrary to our present findings, earlier reports from Ethiopia13 and Philippines27 showed lack of correlation between iron status and goitre rate. Contrary to what has been reported previously12 another component of the present study failed to find difference in goiter reduction between vitamin A + iodine and iodized oil alone supplemented groups. The distribution of vitamin A deficient subjects (nominator) was 11/90 in group A and 12/95 in group B; small were vitamin A deficient. Goiter reduction between the two groups was not significant. This was also further assessed by the in-depth analysis in vitamin A deficient subjects in each intervention groups and yet goitre regression was not significantly different between the two groups. Although not significant, median TSH concentration was relatively lower in vitamin A + iodine supplemented group than iodine alone supplemented group A. Zimmermann et al12 reported that in IDD and VAD affected children receiving iodated salt, concurrent vitamin A supplementation improved iodine efficacy. In the present study, vitamin A supplementation appeared to have no effect on goitre reduction. This might be due to the fact that most children under the investigation were not vitamin A deficient and the sample size was also small. In animal studies, VAD has been reported to impair iodine uptake by the thyroid gland33 and to adversely affect the organification of precursors11 for the formation of the thyroid hormones. Studies on the role of vitamin A on thyroid iodine metabolism are still mixed and hence we suggest further study on the functional interaction of vitamin A and iodine. School survey as well as supplementation results of the present study suggest that iron deficiency has a contributing role for endemicity of goitre in school children. Iron + iodine supplementation seems to play a better role in thyroid function than iodine supplementation per se. Thyroid hormone synthesis is catalyzed by thyroperoxidases which mainly depends on iron availability34. Iron deficiency has an adverse effect on thyroid hormone production thereby increasing TSH level which may be responsible for thyroid gland hyperplasia and hypertrophy35. Deficiency of the three micronutrients VA22 and Iodine20 and iron23 have been a public health problem and coexist affecting children in Ethiopia. Dual supplementation of iron and iodine was found to be effective in goiter reduction than iodine alone. Hence the envisaged IDD intervention programs should take into account iron to combat micronutrient deficiency. It has been reported36 that in malaria endemic areas children at risk of malaria are more likely to die of the disease if they are given dietary supplements of iron and folic acid. In the present study malaria cases were not reported which could be due to distribution of insecticide treated bed nets by Federal Ministry of health. Conclusion The coexistence of vitamin A, iodine and iron deficiencies is reported in school children. According to WHO classification the deficiency rates of these micronutrients indicate severity and public health inference of the problems. Iron + iodine supplementation seems to play a better role in thyroid function than iodine supplementation alone. Hence, the ongoing IDD intervention program should take into account the way how to incorporate iron to control micronutrient deficiency among affected groups. Acknowledgements The authors gratefully acknowledge students, schoolteachers and school committee who gave a large part of their time to participate and facilitate this study. We thank the EHNRI and staff members of the institute particularly the laboratory group; Dilnesew Zerfu, Adamu belay, Israel G.Hiwot, Mengistu G.Tsadik and Alemnesh zilelew for their many contributions in the analysis of the biological samples. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08029t6.jpg] [js08029t1.jpg] [js08029f1.jpg] [js08029t4.jpg] [js08029t2.jpg] [js08029t5.jpg] [js08029t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}