 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
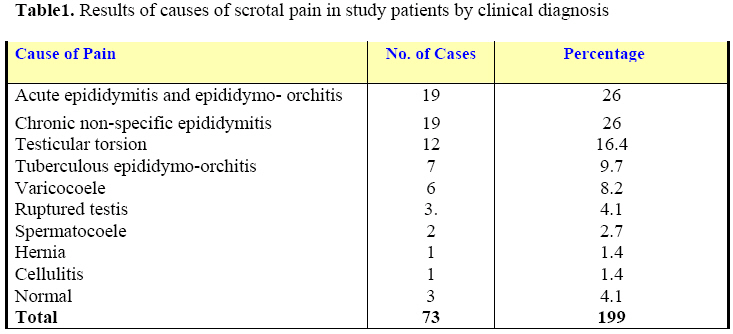
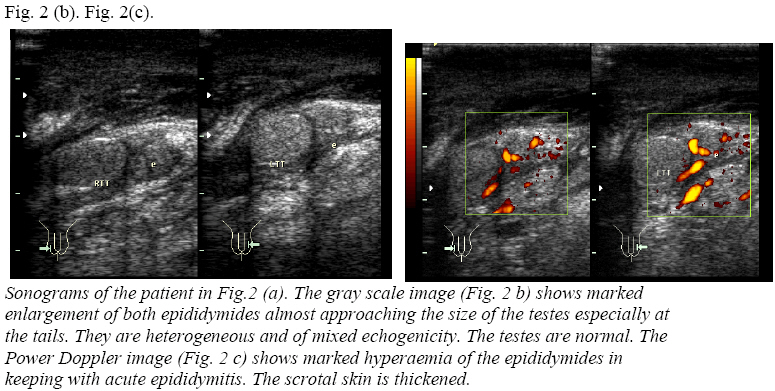
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 68-74 The Sonographic Pattern of Diseases PresentingWith Scrotal Pain At Mulago Hospital, Kampala,Uganda J. Opio1, R.K. Byanyima2, E. Kiguli-Malwadde2, S. Kaggwa3, M. Kawooya2 1Soroti Hospital. Code Number: js08033 Background: Scrotal pain is a common presentation in the male patient. There is a wide overlap of symptoms and signs making differentiation at clinical diagnosis difficult. Ultrasound has been documented to improve the accuracy of diagnosis of scrotal diseases. This study was aimed at determining the sonographically detectable diseases in patients with scrotal pain, describe their sonographic appearances and to relate the diseases to the socio-demographic and clinical characteristics of the patients presenting at Mulago hospital. Introduction There is a wide over-lap of symptoms and signs of scrotal diseases, and because of this, none has a pathognomonic presentation. It is therefore difficult to differentiate these conditions on clinical grounds. For testicular torsion, 25% of patients have a history of gradual onset of pain similar to that seen in epididymitis1 and physical examination may be sub-optimal due to pain and swelling. This scenario greatly hampers clinical differentiation between these two entities whose management approaches are totally different. Before the advent of imaging modalities capable of confirming the cause of acute scrotal pain, immediate surgical exploration was the standard approach when testicular torsion was suspected. This resulted in 50% unnecessary surgical explorations2. In the Sexually Transmitted Diseases clinic at Mulago hospital, many patients present with scrotal pain and receive empirical treatment for epididymitis or epididymo-orchitis on the basis of clinical evaluation. In surgical clinics, patients suspected to have testicular torsion undergo surgical exploration. This increases the chances of misdiagnosis with resultant complications and sometimes need-less surgery. The causes of scrotal pain include epididymitis, epididymoorchitis, testicular torsion, appendicular torsion, trauma, Fournier’s gangrene, testicular vasculitis, testicular tumor with tumor necrosis or haemorrhage into it and idiopathic scrotal oedema. The following were the common causes of scrotal pain on clinical grounds in the year 2002 at Mulago hospital: testicular torsion (55.4%), acute epididymitis and epididymoorchitis (17.4%), infected hydrocele (15.4%), funiculitis (1.5%), and chronic epididymitis (9.8%). Worldwide, scrotal ultrasound has become an excellent non-invasive imaging modality with peculiar attributes such as high sensitivity and ability to characterize and distinguish between intra- and extra-testicular lesions. More accurate diagnoses can be made using ultrasound and the management pitfalls avoided. Patients and Methods A cross sectional study was carried out at Mulago Hospital Department of Radiology between May 2003 and March 2004. Seventy three patients with scrotal pain aged 6 months to 85 years (mean was 31.2 years) were evaluated using scrotal ultrasound following clinical assessment. Consecutive patients who presented with scrotal pain and consented to the study were recruited. The patients with scrotal laceration, history of previous surgery or those who underwent surgical exploration on the basis of clinical assessment were excluded. A record of testicular position and outcome of Prehn’s test, on clinical examination, were entered into the data sheet All the examinations were performed by radiologists using the ATL HDI 1500 machine (model 2000) with a 5-12MHz linear transducer with Doppler capability. The examinations were performed in supine position, in a warm room that afforded privacy. The transducer was covered with protective sheath to prevent contamination. Comparative axial views of both testes were obtained first, and then the sagittal and axial views of each testis and scrotum were obtained and documented. Abdominal ultrasound was performed as well in cases in which the scrotal findings suggested a possible intra-abdominal involvement by the disease. Ultrasound examination aimed at localizing the pathologic lesion within the testis, epididymis or para-testicular tissues, characterizing the lesions in terms of echo-texture, echogenicity and definition of outline, determination of the size and extent of the lesion, determination of the state of perfusion of the testis, epididymis and the lesions by Doppler examination as well as detection of complications like formation of hydrocele, abscess or calcification. Photo documentation was done in the form of hard copy sonograms and floppy discs. Images were also saved in the ultrasound machine computer memory. Image interpretation was done at least two radiologists. Description of the abnormalities detected was done and a diagnosis made on the basis of characteristic sonographic appearances. Epididymal enlargement was categorized as ‘Normal’ (up-to 10mm for the head and 3mm for the body and tail), ‘Moderate’ (11-15mm for the head and 4-10mm for body and tail), ‘Marked’ (more than 15mm for the head and more than 10mm for body and tail). The degree of blood flow within the lesion was also arbitrarily categorized as absent if there was no flow signals detected, reduced compared to the normal, normal if there was a few spotty signals, moderately increased if there were more than a few spotty signals but not grossly hyperemic, markedly increased if there was grossly hyperemic. The clinical, laboratory and radiological data were entered into a data sheet. The final diagnosis was arrived at where applicable by surgical exploration, tissue biopsy for histology, urinalysis and response to antibiotic treatment. Results Seventy three patients with scrotal pain were evaluated. The age ranged from 6 months to 85 years (mean age 31.2 years). The majority of study patients were adults more than 18 years of age (87.7%). Of these, 54.7% were in the 19-29 year age-group. Only 1 patient (1.4%) was less than 5 years old and 10.9% were adolescents. The causes of scrotal pain are summarized in table 1. There was significant associations between scrotal swelling and testicular torsion (p=0.0384) and acute epididymitis (p=0.0351). Significant statistical association was observed between scrotal tenderness and testicular torsion (p=0.0404) and acute epididymitis (p=0.0268). A positive Prehn’s test was not significantly associated with the diagnosis of acute epididymitis or testicular torsion. Transverse testicular position had a significant statistical association with testicular torsion though it was demonstrated in only 4 (33.3%) cases. Sonographic Findings Ten of the 12 patients sonographically diagnosed with testicular torsion were confirmed at surgery. One had spontaneous de-rotation and the parents declined surgery and the last case had had bilateral torsion within a span of three months and was considered beyond redemption. Seven (63.6%) out of the 11 cases suspected to have tuberculous epididymo-orchitis were confirmed at histology, while 1 (9.1%) was reported as chronic non-specific epididymitis and another 1 (9.1%) as acute epididymitis. The other 2 (18.2%) recovered on antibiotics and were finally considered cases of acute-on-chronic epididymitis. All the 3 cases of suspected ruptured testis and 1 case of inguino-scrotal hernia at ultrasound were confirmed at surgery. The final diagnoses of acute epididymitis were made on the basis of blood flow pattern and response to antibiotics. The diagnoses of chronic epididymitis, varicocele and spermatocele were made on the basis of their characteristic sonographic findings only. No lesions were seen in 3 patients. Sixty-two (84.9%) of the patients were found to have disease involving the epididymis and in 11 (15.1%) the epididymis was not involved. Six (50%) patients with torsion had marked epididymal enlargement; 1 (8.3%) had moderate enlargement. The epididymis was of normal size in 5 (41.7%) cases The epididymis was enlarged in all these cases of acute epidydimitis , moderately in 3 (15.8%) and markedly in16 (84.2%).The epididymis was within normal size range in 5(26.3%) cases of chronic nonspecific epidydimitis. It was moderately enlarged in12 (63.2%) and markedly in only 2 (10.5%) one of which followed trauma. The epididymis was markedly enlarged in all the 7 (100%) cases with tuberculous epididymoorchitis while it was moderately enlarged in 2 and markedly in 1 (33.3%) of cases.The epididymis was within normal size range in all cases of spermatocele Significant statistical association was observed between epididymal enlargement and testicular torsion (p=0.0490), acute epididymitis (p=0.0018) and Tuberculous epididymitis (p=0.0247). Spermatocele was associated with a normal size epididymis (p=0.0135). In both torsion and post traumatic testicular rupture the sonographically observed lesions involved both the testis and epididymis in which cases there was significant statistical association (p=0.00029 and p= 0.0141 respectively). The lesions in chronic non-specific epididymitis were commonly located in either the head 8(42.1%) or the tail 7 (36.8%). The whole epididymis was involved in 3 (15.8%) and there was testicular involvement in only 1 (5.3%) case. Significant association was noted with this pattern (p=0.000006). All the spermatoceles were located in the epididymal head and this was a statistically significant finding (p=0.0244). In acute epididymitis, the lesions were most commonly found involving the entire epididymis 9(47.4%) or both the epididymis and the testis 7 (36.8%). This pattern was shared with tuberculous epididymo-orchitis in which the lesions were seen in the whole epididymis in 4 (57.1%) and both the epididymis and testis in 3 (42.9%) cases. There was no significant association in either case. No cases of isolated lesions of the body of epididymis were seen. Extent of lesions: Lesions were classified as either focal or diffuse. The lesions in testicular torsion were all diffuse. In acute epididymitis, 15 (78.8%) cases had diffuse while 4(21.1%) had focal lesions. The above conditions show a statistically significant correlation with diffuse lesions (p=0.0008 and p=0.0347 respectively). Six (85.7%) cases of Tuberculous epididymoorchitis had lesions that were focal in nature and the correlation was statistically significant (p=0.0176) Size of focal lesion: The diameters of the focal lesions were measured and categorized into 3 groups. Five (83.3%) cases of tuberculous epididymo-orchitis had focal lesions greater than 10mm in diameter, reflecting a significant statistical correlation (p=0.0318). Tuberculous lesions also had the widest mean diameter (15.7mm). Only 4(21%) cases of acute epididymitis had focal lesions. Three (75%) of them had focal lesions greater than 10mm but there was no significant statistical association (p= 0.2142). A majority of cases of Varicocele (83.3%) were of diameter less than 5mm. Only in 1 (16.7%) was it more than 10mm. A significant correlation was observed (p=0.0024) Outline of Lesion: All cases of testicular torsion had ill-defined lesions. Sixteen (84.2%) cases of acute epididymitis also had ill-defined lesions. In both conditions above, the associations were significant (p=0.0025 and p=0.0240 respectively). A majority of tuberculous lesions (85.7%) were well-defined and there was a significant statistical correlation (p=0.009). All varicoceles were well-defined and there was a significant association here as well (p=0.0016). Although a majority of chronic epididymal lesions were ill-defined (63.2%), there was no significant association observed. Echogenicity and Heterogeneity of the Lesion: All lesions observed were either Hypoechoic or of mixed echogenicity. Purely hyperechoic lesions were not seen. There was no statistically significant association between the echogenicity and cause of any of the lesions. Apart from varicocele and spermatocele lesions which were mainly homogeneous and therefore had significant statistical correlations (p=0.0002 and p=0.02278 respectively), the rest of the lesions were predominantly heterogeneous and had no significant correlations. Blood flow Pattern: Statistically significant correlation was seen between absent blood flow and testicular torsion (p=0.0000), normal or moderate flow and chronic epididymitis (p=0.00067), moderate flow and tuberculous epididymo-orchitis (p=0.019) and marked blood flow in acute epididymitis/ epididymo-orchitis (p=0.000002). Presence of Hydrocele: Hydrocele was present in some cases of testicular torsion (33.3%), acute epididymitis/ epididymo-orchitis (52.6%), chronic epididymitis (42.1%), most cases of tuberculousepididymo-orchitis (71.4%) and in all cases of testicular rupture (100%).Testicular rupture was significantly associated with the presence of hydrocele (p=0.072), and varicocele with its absence (p=0.0351). No associations were observed with the other lesions. Echoes in hydrocele: Hydrocele was categorized as either clear or having internal (speckled) echoes or septations. The highest proportion of clear hydrocele was observed in chronic nonspecific epididymitis (50%). There was a significant statistical association between chronic epididymitis and the nature of the hydrocele (p=0.0363). No significant association was observed between hydrocele and other conditions. Presence of calcifications: Calcifications were observed in 1 case of acute epididymitis, 2 and 5 cases of chronic epididymitis and tuberculous epididymo-orchitis respectively. There was a strong statistical association between calcifications and tuberculous epididymo-orchitis (p=0.0008). Abdominal Ultrasound findings: Prostatic enlargement was seen in 2 patients with acute epididymitis and 1 with chronic epididymitis. All of them were over 60 years of age. Unilateral renal parenchymal cavities were seen in 2 patients with tuberculous epididymitis and 1 with varicocele. Comparison of clinical and Sonographic diagnoses with Final diagnoses: This was done to try to establish the reliability of clinical assessment compared to sonographic evaluation. Torsion: Twelve patients were clinically suspected to have testicular torsion. Only a third proved to be cases of torsion at final diagnosis, 7 of acute epididymitis, and 1 of chronic epididymitis (table 8). The sensitivity of clinical assessment in detection of testicular torsion was 33.3%; the specificity was 86.9% and its positive predictive value was also 33.3%. Torsion and necrosis. There is diffuse enlargement of the left testis and epididymis which are also heterogeneously hypo-echoic. Power Doppler scan shows normal flow in the right testis but no flow in the left testis Surgical specimen of the patient, shows testicular and epididymal necrosis. Sonograms of the patient in Fig.2(a). The gray scale image (Fig.2(b)) shows marked enlargement of both epididymides almost approaching the size of the testes especially at the tails. They are heterogeneous and of mixed echogenicity. The testes are normal. The Power Doppler image (Fig. 2 c) shows marked hyperaemia of the epididymides in keeping with acute epididymitis. The scrotal skin is thickened. Acute epididymitis: Six patients were clinically suspected to have acute epididymitis. Four of them proved to be cases of testicular torsion, 1 of tuberculous epididymo-orchitis andonly 1 of acute epididymitis at final diagnosis. The sensitivity of clinical assessment in detection of acute epididymitis was 5.3%; the specificity was 90.7% and its positive predictive value was 16.7%. The accuracy of clinical assessment in detecting and differentiating between testicular torsion and acute epididymitis was very low. The sensitivity of ultrasound in detection of testicular torsion was 100%. Its positive as well as negative predictive values were also 100%. The sensitivity of ultrasound in detection of acute epididymitis was 84.2%. Its specificity was 100% and the positive predictive value was also 100%. The sensitivity of ultrasound in for detection of tuberculous epididymo-orchitis was 100%; its specificity was 92.7% and the positive predictive value was 63.6%. The sensitivity and specificity of ultrasound for detection of ruptured testis were both 100%. DiscussionScrotal pathology is common and affects a wide age range of patients, although the young adults in early reproductive age are the ones commonly affected in our population. The sexually active age group is most vulnerable and it has been documented that sexually transmitted organisms are the commonest cause of infection in young adults3. The second peak at 50-60 years is explained by acquired genito-urinary lesions especially prostatic enlargement predisposing to infection. Although testicular torsion was seen in almost all age-groups, its incidence dropped after the 19-29 year age range. Tolia and Mewman4 also documented testicular torsion in men older than 40 years, however we noted two distinct peaks of incidence the newborns and teenagers between 12 and 18 years of age. It has been reported that Prehn’s sign may differentiate acute epididymitis and torsion. When positive, the pain from infection is relieved by elevation of the scrotum above the symphysis pubis but worsens if it is testicular torsion. Starvos Atet al reported that this statement is untrue in many patients1. The findings in this study are in agreement with Starvos’ report .This may be because the physical examination is usually sub-optimal in most cases due to severe tenderness associated with both conditions. Transverse position is usually associated with torsion and is directly related to the degree of torsion. However, this means that the testis may be of normal position in lesser degrees of torsion, thereby increasing the chances of missing any torsion.Quite often the degree of scrotal swelling and pain prohibits accurate delineation of the testis and therefore makes the sign unreliable. There was no significant statistical difference in terms of epididymal enlargement, between torsion and acute epididymitis (p=0.5619), nor was any observed between acute epididymitis and tuberculous epididymitis either (p=0.5396). Varicoceles, spermatoceles, ruptured testis and inguino scrotal hernia can be confidently at ultrasound and require no other confirmatory test. Tuberculous epididymo-orchitis and chronic non specific epididymo-orchitis give focal lesions that tend to be larger in the former. Acute epididymo-orchitis gives diffuse lesions. Yang et al3 got similar results and noted that this may be due to the aggressive and faster spread of acute infections compared to chronic infections. There was no statistically significant association between the echogenicity and cause of any of the lesions. There was significant association between calcificationa and tuberculous lesions. Wolf et al6 described calcifications as highly suggestive though non specif for tuberculous epididymo-orchitis. The characteristic sonographic featuresof tuberculous Epididyno-orchitis as described by Yang et al3 include marked epididymal enlargement, large well defined lesions without corresponding degree of hyperaemia and presence of calcifications. No case of tesiticular tumour was encountered in this study probably because testicular tumours are painless unless complicated by haemorrhage or necrosis7. Conclusion Infections and testicular torsion are the commonest causes of scrotal pain in patients presenting in Mulago Hospital. Non-tuberculous epididymal and testicular infections are related to sexual activity in the young adults and to genito-urinary abnormalities in the pre-pubertal and elderly individuals. Sonographic imaging was found to improve diagnostic accuracy in evaluation of patients with scrotal pain at Mulago hospital. Conditions that require urgent or specific therapy like testicular torsion, acute epididymitis, ruptured testis and tuberculous epididymo-orchitis can be depicted at ultrasound with high degree of accuracy. None of the patients presenting with with scrotal pain at Mulago Hospital during the period under review had testicular tumour. ` References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08033f2.jpg] [js08033t1.jpg] [js08033f1.jpg] |
| |||||||||

{kind=link}
{kind=link}