 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
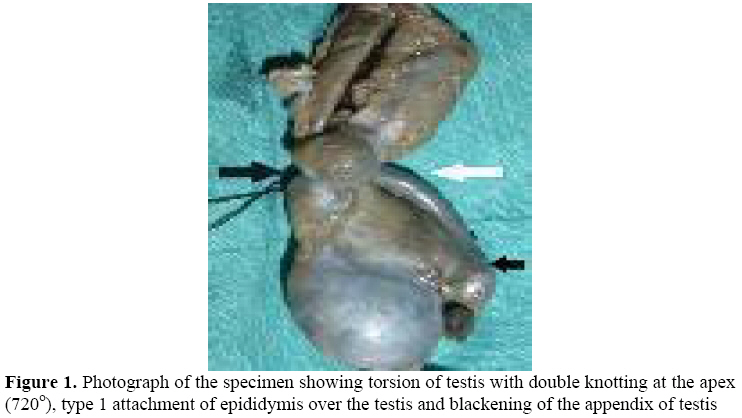
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 75-76 Torsion of testis in an adult: presenting as scrotal mass with minimal discomfort S. Dwivedi1, S.R. Joharapurkar2, K.B. Golhar3 1Associate Professor in Surgery, Department of Surgery, Code Number: js08034 Testicular torsion in adulthood is relatively unusual and has a higher morbidity rate. We present a case of 26-year-male patient presented with gradually progressive enlargement of left scrotum associated with minimal local and abdominal discomfort for last two months. Investigations and intra-operative findings were suggestive of testicular torsion. We report this case because of its unusual painless presentation and this emphasizes the importance of emergent management for scrotal lesions through public education to avoid delayed presentation to medical facilities. Introduction Testicular torsion in adulthood is relatively unusual and has a higher morbidity rate, and the successful management of such patients depends on; early consultation on the part of the patient, correct diagnosis by the doctor at first consultation and urgent surgical exploration of the affected testis1,2 Case report A 26-year-male patient presented with gradually progressive enlargement of left scrotum associated with minimal local and abdominal discomfort for last two months. His general and systemic examination was unremarkable. On local examination there was palpable, 6x8 cm hard testicular swelling with preserved testicular sensations. Overlying scrotal skin was free and there was no local rise of temperature. There was slightly thickened and tender left spermatic cord. Hematological investigations were normal except mild leucocytosis. Urine examination was normal. Ultrasound and colour Doppler scrotum was suggestive of torsion of left testes and there were no sign of viability. Opposite testes and intra-abdominal examination was normal. On exploration there was intra-vaginal left testicular torsion with double knotting of 720 degree at the apex and nonviable testes. The epididymis was attached to the testes at the head and tail only (Type-1) (Figure - 1). A high left orchidectomy was performed. The patient was doing well at follow up. Discussion Testicular torsion occurs due to anatomic anomalies of tunica vaginalis and epididymis that allow excessive testicular mobility inside the scrotum and intravaginal torsion (bell clapper deformity) being the most frequent type1,3. Medial rotation that ranges from 360º to 720º in its own axis can cause interruption of the organ’s vascularization as in present case (rotation of 720o) 1,3. 1,3 In addition our patient had Type I attachment (only head and tail of epididymis attached to the testes) 4. The diagnosis is made mainly through clinical examination and signs and symptoms of torsion include acute scrotal pain and testicular ascent, and the testis can lie horizontally with or without inflammatory signs5,6. However, in doubtful cases Doppler ultrasonography of the spermatic cord and testicular scintigraphy can be used to assess testicular perfusion6,7. When these tests are not promptly available, thus in doubtful cases following clinical examination, when complementary exams cannot be performed, urgency scrotal exploration is the treatment of choice and no investigation substantially improves clinical diagnosis enough to warrant any delay in definitive surgical intervention1,3, 5,8. Testicular torsion can occur at any age and for males aged 1 to 25 years, testicular torsion is more common than testicular tumors, and increasing age is the sole identifiable risk factor for orchiectomy1,7. The testis will present irreversible damage if the torsion is not resolved within up to 6 hours1. We report this case because of its unusual painless presentation and this emphasizes the importance of emergency management for scrotal lesions through public education to avoid delayed presentation to medical facilities. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08034f1.jpg] |
| |||||||||

{kind=link}