 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
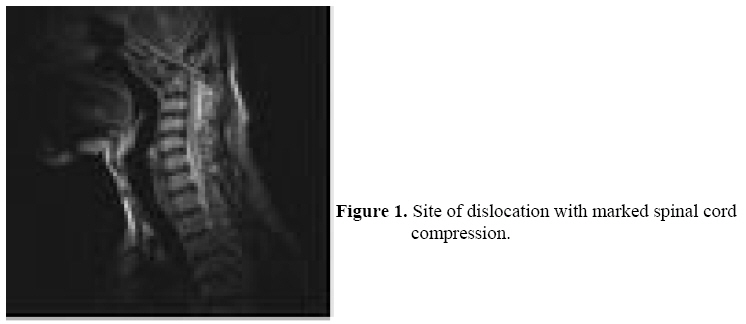
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 77-78 Cervical myelopathy from traditional bonesetters’ treatment of spinal injury O.E. Idowu1,2, O.C. Idika2, R.A. Apemiye2 Neurosurgery Division, Department of Surgery, 1Lagos State University College of Medicine and 2Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria Correspondence to: Dr. O.E. Idowu, E-mail: oeidowu412@yahoo.com Code Number: js08035 Continuous beliefs in traditional bone setters (TBS) and traditional healers remain rife in the sub-Saharan African1. The morbidity, mortality and financial loss resulting from patient management by this sect of health providers are still a burden in our society. Atlanto-axial joint is the most complex joint of the body. Approximately 55% of the entire rotation of the cervical spine takes place at this joint2. This joint is kept stable only by its capsule and ligaments, hence the possibility of dislocation. Any injury in this region is associated with potentially catastrophic neurological complications. We report a case of severe upper cervical spinal cord compression resulting from a mismanaged atlanto-axial disruption by a TBS. Case report M.C. was a 44-year- old male university graduate, businessman who presented with one and a half year history of slowly progressively worsening post-traumatic weakness and sensory impairment in all limbs and 2 weeks history of faecal and urinary incontinence. His weakness was worse in the lower extremities, likewise the sensory deficit. There was associated torticollis and neck pain. The trauma was due to a passenger road traffic crush with mild head injury. Following the accident, he had transient quadriparesis for about 4 hours while at a tertiary Hospital. When he was informed of a possible spinal injury which needed further imaging, he refused further treatment in the Hospital, and opted for a traditional management option based on his strong belief in TBS’s treatment of bony injuries. Following the onset of bisphicteric incontinence, some of his relations prevailed on him to try another tertiary Hospital. Examination at presentation revealed a middle aged man in respiratory distress. Examination of his mental status was normal. Muscle bulk was reduced in all limbs but worse in the lower extremities. Spastic quadriparesis with sustained clonus was noted (upper extremities power grade 3, Lower extremities power grade 2). His sensory level to pain and temperature was C2. There was faecal and urinary incontinence. Other systems were normal. A clinical diagnosis of C2 myelopathy (Di Lorenzo grade IV- Totally dependent) secondary to mismanaged cervical spine injury was made. Cervical spine radiographs revealed atlanto-axial dislocation with marked spinal canal narrowing and bony union of C1/C2 anteriorly. Magnetic resonance imaging showed severe cervical spinal cord compression from the dislocated atlanto-axial dislocation (Fig 1). Mantoux test was negative. Erythrocyte sedimentation rate and full blood count were normal. He subsequently had posterior decompression in the form of excision of the posterior arch of the atlas and posterior occipitoaxial arthrodesis. Post-operative period was uneventful. Patient improved significantly neurologically becoming ambulant with walking support, and continent of urine and faeces. Discussion Disruption of the atlanto-axial joint may reduce the diameter of the spinal canal to 10mm or less, causing compression of the spinal cord3. Nevertheless, injury to the spinal cord in survivors is rare4. Early intervention is the critical factor for a satisfactory outcome. However, delayed diagnosis can result in catastrophic consequences, including neurological deficits, cosmetic deformity and, in rare instances, paralysis and death. For survivors of this disruption, early closed manipulative reduction with spinal cord monitoring, followed by external bracing, restores both normal anatomical relationships and mobility in many patients. In some patients, however, the manoeuvre fails, and open reduction and fixation is necessary. If treatment is delayed, as in this case, bony union occurs and hence open reduction and fixation becomes mandatory. The morbidity if not mortality and financial loss resulting from the management by traditional bonesetters is still real in our society. Cultural beliefs are still a major factor that draws patients to these quacks. Education and strong legislation is advocated against TBS. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08035f1.jpg] |
| |||||||||

{kind=link}