 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 101-104 Otolaryngological Practice in Developing Country: A Profile of Met and Unmet Needs A.O. Lasisi Senior Lecturer/Consultant, Department Of Otorhinolaryngology, College Of Medicine,
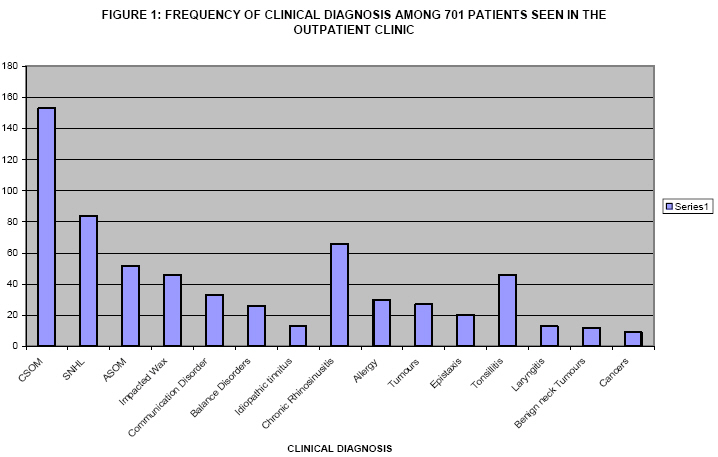
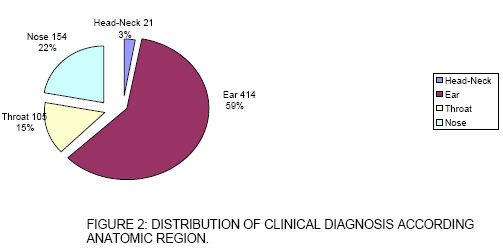
University Of Ibadan, Ibadan, Nigeria. P.O. Box 22040, University of Ibadan, Code Number: js08041 Background: There has been a significant advance in the practice of otorhinolaryngologic surgery from the simple excisional surgery to minimally invasive functional endoscopic techniques, reconstruction and the use of laser. In this review we present our experience of the otolaryngologic practice in Nigeria Introduction The practice of otorhinolaryngologic surgery has advanced from the simple excisional surgery to minimally invasive functional endoscopic techniques, reconstruction and the use of lasers1,2. Accompanying these are various forms of plastic repair of the ear, nose and throat region making the regain of physiologic function a realizable surgical goal. This has thus made the specialty technology – intensive and dependent on equipment such as operating microscopes, sinus endoscopes, surgical navigators and various implants among others1,2. Unfortunately, this does not seem to be so in the sub-Saharan Africa where otolaryngologic practice is still at the infantile stage. This has resulted in the sparcity of data on otorhginolaryngologic practice from the sub region. This article reports the analysis of 701 patients seen in our practice in 4 years highlighting the spectrum and peculiarities of E.N.T diseases, surgical management and its limitations and identifying research issues which could help in management. Patients and Methods This was a retrospective analysis of 701 patients seen in the Outpatient Consultation Clinic within the last 4 years in one of the biggest tertiary centre in Nigeria. The records of cases seen from the year 2000 to 2004 were computerized; this allowed for easy retrieval and analysis. The basic biodata, clinical features, diagnostic and therapeutic modalities were extracted and analyzed using simple statistics. The results of distribution of clinical diagnosis among the 701 cases and 111 surgical procedures are presented. Results Seven cases were excluded from the study for inadequate information. Clinical records of 701 patients were found suitable for analysis out of 708 cases seen from December 2000 to December 2004 at the Otorhinolaryngology Clinic of the University College Hospital, Ibadan, Nigeria. The ages ranged between 3 months and 77 years (mean = 24.3, SD =18). There were 358 males and 350 females (M;F ratio = 1:1). Chronic suppurative otitis media was recorded in 153 (22%) of the patients followed by sensorineural hearing losses in 84 (12%). Inflammatory disorders of the sinuses and larynx accounted for 112 (14%) while head and neck cancers were recorded in 9 (1.3%) of the cases Figure 1. In all, ear pathology was responsible for 414 (59%) of outpatient attendance followed by rhinology in 154 (22%), laryngologic cases in 105 (15%) and lastly head and neck cases 21 (4%). Operative procedures were performed for 111 (16%) only. Modified radical mastoidectomy and tympanoplasty was the most frequent surgical procedure accounting for 19 (17%). This was followed by intranasal antrostomy in 16 (15%), rigid oesophagoscopy for removal of foreign bodies in 9 (8%), caldwel-luc antrostomy in 8 (7%), adenoidectomy in 7 (6%) and tonsillectomy in 7 (6%) patients. Endoscopic sinus surgery and fibreoptic laryngo-oesophagoscopy were done in 4 (5%) patients (Figure 2). Analysing the surgical procedures according to the divisions, laryngologic/head and neck surgery accounted for 47 (42%), rhinologic 31 (28%), otologic 29 (26%) and minimal invasive / endoscopic surgeries 4 (4%). The diagnostic facilities were inadequate. Only pure tone audiometry was available for investigating hearing losses, cochleography, otoacoustic emission and auditory brainstem response were not available. Hearing aid was affordable by only 3 (4%) out of the 84 patients with hearing loss, the rest were referred to special schools for training. Out of 79 patients requiring computerized axial tomography scanning for investigation of intracranial and skull base involvement of the lesions, only 12 (15%) could afford it. Hence management was based on plain radiography of the paranasal sinuses and temporal bone. Only nasal smear eosinophil was used to investigate nasal allergy, there were no facilities such skin sensitivity test. Discussion Chronic suppurative otitis media and sensorineural hearing loss constituted more than one – third of patient seen in the outpatient consultation. This high prevalence of chronic ear infection is contrary to the reports of advanced countries3. This is probably due to a combination of inaccessibility to health care facilities, local customs and beliefs, harmful traditional practices and poor treatment of acute cases by the first contact health personel4,5. The predominant proportion of open mastoidectomy in the treatment suggests a high rate of complicated cases of cases seen. The aetiologic/risk factors identified included recurrent upper respiratory tract and sinus infections, overcrowding and immunodepression. Otitis media with effusion from eustachian tube dysfunction due to adenoid enlargement as reported in the West has not been typically seen in our patients. It is possible that the cases were not presented to us at this early stage. Furthermore, this was attributed to the dry sub-Saharan climate which is not conducive to the growth of spores, allergy and otitis media with effusion and suggested research into racial and genetic factors6. The indication for adenoidectomy has been severe upper airway obstruction leading to snoring and excessive daytime hypersomnolence. The hearing losses were mostly congenital; the acquired cases were sequelae of viral infections and complications of meningitis. Many of these cases need genetic screening, viral culture and facilities to differentiate sensory from neural hearing losses, this will help in identifying the suitability for cochlear implantation and counseling. Unfortunately these are not available in our centre. Most of the procedures consist of open (excisional) surgeries: caldwel-luc antrostomy, lateral rhinotomy, frontoethmoidectomy, tonsillectomy and neck dissection. The indications for these procedures were nasal polyposis, invasive fungal swellings, inverted papilloma and pyomucocoeles. These indications are similar to the other authors7,8. The three endoscopic sinus surgeries were done following the introduction of sinus endoscopes into our hospital recently; further training of the staff may be needed for this to become established. It is remarkable that the number of surgeries does not reflect the outpatient consultation. While otology constituted 59% of outpatient consultation, laryngologic surgery was highest 39% followed by nasal and ear surgeries 28% and 26% respectively. The procedure mostly needed by the CSOM patients after achieving a dry ear with aural dressing is simple tympanoplasty. An estimated 1000 patients was reported earlier waiting for tympanoplasty however this could not be done due to absence of microsurgical facility, hence the reduction in otologic surgery5 (Lasisi et al 2002). Conclusion The study showed that there was a considerable patient-load with inadequate diagnostic and therapeutic facilities when compared with contemporary practice worldwide. This is similar to the experience of Murphy6 in Ghana. It is our impression that addressing a change in this trend will require facilitated access to healthcare facilities, provision of diagnostic and operating equipment in most centres and specialized training of surgical personnel. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08041f3.jpg] [js08041f2.jpg] [js08041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}