 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
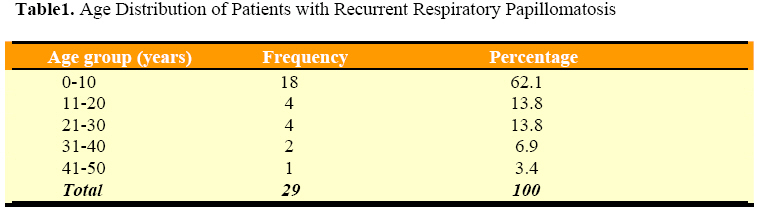
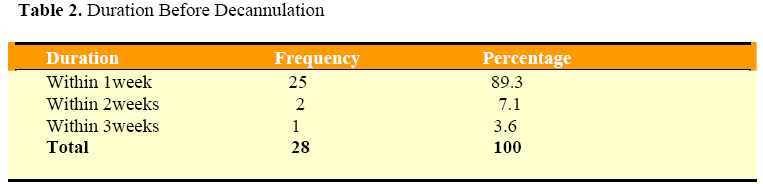
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 105-108 Recurrent Respiratory Papillomatosis in Jos, Nigeria: Clinical Presentation, Management and Outcome A. A. Adoga1, L. T. Nimkur1, A. S. Adoga1, 1Lecturer/Otorhinolaryngologist, Otorhinolaryngology Unit, Department of Surgery, Jos University Teaching Hospital, Pmb 2076, Jos, Plateau State, Nigeria. Code Number: js08042 Background: Recurrent respiratory papillomatosis is a benign neoplastic disease of viral aetiology which can have significant morbidity or mortality and presents great challenges in it management. This study evaluates our experience with the management of this disease. Introduction Recurrent respiratory papillomatosis is a benign neoplastic disease characterized by warty-like lesions occurring anywhere along the aerodigestive tract and caused by the Human Papilloma virus (HPV) of which 90 subtypes has been described1. HPV types 6 and 11 are responsible for papilloma in the airway2. Two clinical forms of the disease occur, the juvenile-onset recurrent respiratory papillomatosis (JORRP), an aggressive form and the adult-onset recurrent respiratory papillomatosis (AORRP), which is less aggressive, the former being commoner3. It is a potentially devastating disease exhibiting high recurrence and can have significant morbidity presenting with hoarseness or result in mortality due to airway compromise or less commonly malignant transformation4- recurrent respiratory papillomatosis is an acknowledged risk factor for pulmonary squamous cell carcinoma5. Surgical debulking is the foundation of treatment with endoscopic laser surgery being the current mainstay of treatment6. However, newer surgical techniques utilizing powered microdebriders are taking the place of carbon-dioxide laser ablation7. Research studies are ongoing investigating adjuvant medical therapies such as oral indole-3-carbinol8, intralesional cidofovir injections9 and lymphoblastoid interferon10 amongst others. No safe adjuvant therapy is currently available7. Tracheostomy in the management of recurrent respiratory papillomatosis is controversial, with advocates11 and those who recommend its avoidance if possible as distal viral spread to uninvolved respiratory mucosa could occur12. This group also suggests early decannulation if tracheostomy is unavoidable. Iatrogenic airway stenosis, posterior glottic stenosis13 and glottic webs14 may also occur post-operatively. We present the clinical presentation findings, management and outcome of patients with recurrent respiratory papillomatosis treated over a 10 year period in the Jos University Teaching Hospital, Jos, Nigeria. Patients and Methods Following approval from the Ethical Clearance Committee of our institution, the medical records of consecutive patients presenting to our hospital with recurrent respiratory papilloma within the period August 1997 to July 2007 was analyzed for age, sex, clinical presentation, management profile and outcome of treatment. The results are presented in simple descriptive form and tables. Results Twenty nine patients aged between 2 months and 45 years were managed for respiratory papilloma within the study period. There were 21(72.4%) males and 8 (27.6%) females, giving a male: female ratio of 2.6:1. The highest incidence (62.1%) of this disease was seen in children less than 10 years of age (Table 1). All the patients had histological confirmation of recurrent respiratory papilloma. The presenting features were hoarseness in all the patients and dyspnea in 28 (96.6%) of the cases. Twenty three (79.3%) patients presented within 10 months of onset of symptoms and 6 (20.7%) patients after this period. All but one patient, a 37 year old male, had emergency tracheostomy. Twenty five (89.3%) of these patients were decannulated within 1 week of insertion of tracheostomy tubes, 2 (7.1%) patients within 2 weeks and 1 (3.6%) patient within 3 weeks (Table 2). No patient had evidence of distal viral spread to uninvolved respiratory mucosa. All the patients had direct laryngoscopy and clearance with relief of symptoms. The commonest site of lesions was the vocal cords in 16 (55.2%) patients and the anterior commissure in 13 (44.8%) patients. Follow-up revealed recurrence in two patients who had one repeated episode of direct laryngoscopy and clearance each, giving a recurrence rate of 6.9%. There was no case of post-operative airway stenosis, glottic web and no malignant transformation recorded. Discussion Recurrent respiratory papillomatosis is a potentially devastating benign neoplastic disease of viral etiology which can have significant morbidity or result in mortality and present great challenges in its management. Like in a previous study in Ibadan, Nigeria15 the incidence of this disease is higher in the under 10 age group. Our study still reports the vocal cords and the anterior commissure as the commonest sites of recurrent respiratory papillomatosis.We recorded a relatively low recurrence rate of 6.9% compared to other documented studies4,15. Post-operative complications such as airway stenosis13 and glottic webs14 may occur. Our study reports no case of complications following surgery and there was no malignant transformation recorded. Though endoscopic laser surgery remains the mainstay of treatment of recurrent respiratory papillomatosis, our study shows that in the absence of such a facility e.g. in health institutions of developing countries like Nigeria, the conventional endoscopic surgical excision of this lesion can be done with minimal or no complications and that tracheostomy when needed to relieve upper respiratory obstruction is advocated in the management of these patients. Acknowledgement The authors are grateful to Dr. L. Chirdan of the Pediatric Surgery Unit of the Department of Surgery, Jos University Teaching Hospital for allowing the use of his patient for this study and Mr. Miri of the Medical Records Department of the Jos University Teaching Hospital for his assistance in the retrieval of patients’ case notes. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08042t1.jpg] [js08042t2.jpg] |
| |||||||||

{kind=link}
{kind=link}