 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 109-113 Abdominal Wall Hernias in Upper Egypt: A Different Spectrum. S. A. Ammar1, T. Ismail2 . 1Department of Surgery, 2Public health and Community Medicine Department., Assiut University,
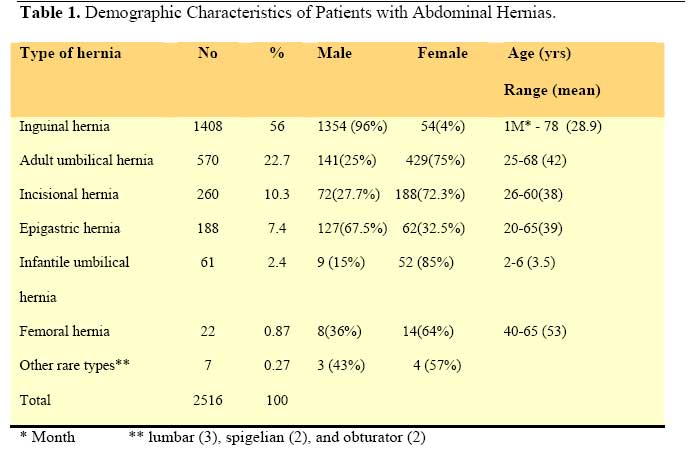
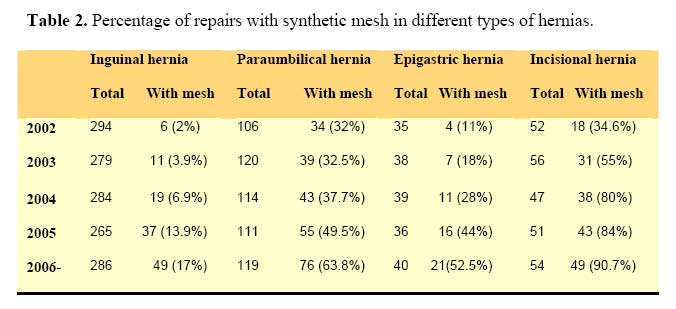
Hospitals, Assiut- Egypt. Code Number: js08043 Background: Hernia is a very common surgical condition affecting all ages and both sexes. To describe and find the possible differences in the spectrum of abdominal hernias and document trends in their management, we carried out a descriptive study of all patients with abdominal hernias admitted to a single tertiary institution during a five years period. Introduction Hernia is literally a weakening or tear in the wall of the abdomen. The name of a hernia is related to its anatomical location. The only way to stop hernia progress is to repair the defect surgically. Hernias are a leading cause of work loss and disability and are sometimes lethal. The danger of a hernia is the possibility that a portion of the intestine become entrapped and strangulated, leading to a surgical emergency 1, 2. Hernia repair is one of the most common general surgical procedures performed worldwide. In the United States and Europe alone, more than a million inguinal hernia repairs are performed annually 3. Most of the figures in textbooks related to epidemiological surveys of abdominal wall hernias are from work done in western countries. In Egypt, a different spectrum of abdominal hernias was noticed. In addition to differences in social habits, nutritional state, and body habitus, certain diseases as liver diseases are more prevalent in Egypt 4-6. These factors predispose to a different spectrum of abdominal hernias. The objective of this study is to find possible differences in the spectrum of abdominal hernias and document local experience in their management. Patients and Methods This study is a descriptive study of all cases of abdominal wall hernias admitted to Assiut University Hospital, Assiut, Egypt from Jan. 2002 to Jan. 2007. Assiut University Hospital (3000 beds) is a big tertiary centre for the entire Upper Egypt. For treatment of inguinal hernia in adults, Bassini-Shouldice or open mesh repair were used. For ventral hernias, the repair ranged from anatomical repair, darning, to open mesh repair. The choice to use mesh in hernia repair depends on size of the defect, weakness of musculature, and surgeon preference. No laparoscopic hernia repair was done since laparoscopy in our centre is almost restricted to laparoscopic cholecystectomy. Data collection was done using the medical records of patients that were included in the hospital archives. Variables included age, sex, final diagnosis and type of repair. Revision of data and coding of variables was done to be ready for computer entry. Data entry and management took place using the Excel program. Statistical analysis and tabulation were done. Descriptive statistics as frequencies, percentages, range, and mean were used. Graphic presentations were done using the Excel program. Results Between Jan. 2002 and Jan 2007, 2516 abdominal hernia repairs were recorded (Table 1). Inguinal hernias were the most common (56%), followed by paraumbilical hernia (22.7%), incisional hernia (10.3%), epigastric hernia (7.4%), infantile umbilical hernia (2.4%) and femoral hernia (0.87%). Other rare types including lumbar, spigelian and obturator hernias represented 0.27%. By far adult umbilical hernia is the most common hernia in women followed by incisional hernias (429 and 188 cases in order). Females underwent more than three times as many inguinal herniorrhaphies as femoral repairs (54 versus 14 cases respectively). 96% of inguinal hernia operations were performed on males. 75% of adult umbilical hernia repairs were done for women versus 25% for men. Epigastric hernias were twice more common among males than females (67.5% versus 32.5% respectively). Excluding the incisional hernias, inguinal hernias constituted 62.4% of spontaneous external abdominal hernias (Figure 1). Adult umbilical hernias represented 25.2% while epigastric hernias represented 8.3%. Femoral hernias represent only 1% of spontaneous abdominal hernias and 1.5% of groin hernias. There were 176 operations (7%) for recurrent hernias. Recurrent paraumbilical hernias were the most common. The rate of recurrent hernias were 14% for paraumbilical, 5.3% for incisional, 4.6% for inguinal and 4% in epigastric hernias respectively (Figure 2). Regarding emergency surgery, 136 (9.6%) of patients with inguinal hernias had surgery for complicated hernia. For ventral hernias, 97 (17%) of patients with adult umbilical hernias and 20 (7.7%) of patients with incisional hernias had emergency operation because of hernia complications. Concerning the use of synthetic mesh in hernia repair, there is an increasing trend towards mesh repair in different hernia varieties (Table 2). Synthetic meshes were most commonly used in the repair of incisional and paraumbilical hernias. The use of mesh in repair of paraumbilical hernia has increased from 32% in 2002 to 63.8% in 2006. For repair of incisional hernia, the use of mesh repair has increased from 34.6% in 2002 to 90.7% in 2006. Regarding mesh repair in inguinal and epigastric hernias, they increased from 2% and 11% in 2002 to 17% and 52.2% in 2006 respectively (Fig. 3). Discussion Documentation of local practices is important. It records not only what is being done, but also what is not being done, and thus helps to identify change and improvement. A number of researchers have conducted surveys to study the spectrum of hernias and trends in their management in their own countries3,7-10. We conducted this study to identify and document the spectrum of abdominal hernias and the repair practices of general surgeons in a major surgical centre in Upper Egypt. Umbilical hernia defects are not uncommon among adults and are believed to be an acquired disease in more than 90% of cases. Predisposing factors include extreme obesity, multiparity, ascites, and large abdominal swellings11,12. In literature, umbilical hernia comprises 3-15% of abdominal hernias13-15. In the present study, the adult umbilical hernia constituted 22.7% of abdominal hernias and notably the most common hernia in women (53.4%). Early marriage and repeated pregnancy may be partially responsible for this relatively high percentage of adult umbilical hernias. Estimates of the frequency of epigastric hernia in the general population ranged from 3-5% 1. In our study epigastric hernias constituted 7.4 % of abdominal hernias and 67.5% of it occurred among males. Egypt is characterized by high prevalence of chronic liver illness, which may predispose to epigastric and adult umbilical hernias. Viral hepatitis together with Schistosomiasis are the major causes of chronic liver disease and liver cirrhosis in Egypt, and both infections are more prevalent in males4-6. Seventy five percent of all abdominal wall hernias are found in the groin1. In our study groin hernias constituted 56.87% of abdominal wall hernias, including incisional hernia, and comprise only 8.5% of abdominal wall hernias in females. In a survey of groin hernia in Denmark, femoral hernia constituted 4% of groin hernias 7 and in Uganda femoral hernia constituted 6.3% of groin hernias16. In other publications, femoral hernia may constitute up to 8.5% of abdominal wall hernias13. In the present study, femoral hernia constituted less than 1% of all abdominal hernias and 1.5% of groin hernias. In the past decade the outcomes of surgery for abdominal wall hernias, in particular midline hernias, have been improved dramatically by the use of prosthetic mesh 17. We noticed expansion in the use of synthetic mesh in hernia repair. Mesh repair in adult umbilical and incisional hernias had increased from 32% and 34.6% in 2002 to 63.8% and 90.7% in 2006, respectively. For inguinal hernia, mesh repair increased from 2% in 2002 to 17% in 2006. In Norway, Mjaland et al reported that the use of mesh in inguinal hernia repairs increased from 1% in 1990-91 to 78% in 200313. In many surgical centres, the most commonly used technique in the treatment of inguinal hernia is mesh repair7-9, 18. In contrast, Odula and Kakande reported that modified Bassini's repair was performed on the majority of inguinal hernias (68.2%) and mesh hernioplasty was not used in inguinal hernia repair in the whole series16. Conclusion The spectrum of abdominal wall hernias differs from one country to another according to prevalence of the predisposing factors for each type in the country. There is increasing trend among surgeons towards using synthetic mesh in hernia repair, which may reflect increasing surgeons trust in mesh repair. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08043t1.jpg] [js08043f2.jpg] [js08043f1.jpg] [js08043f3.jpg] [js08043t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}