 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
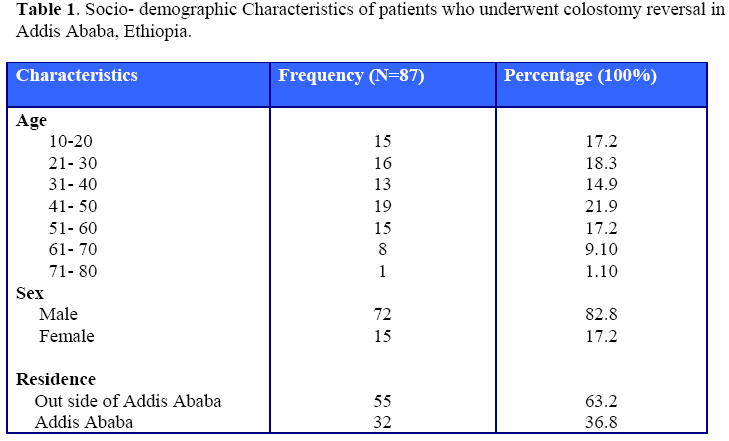
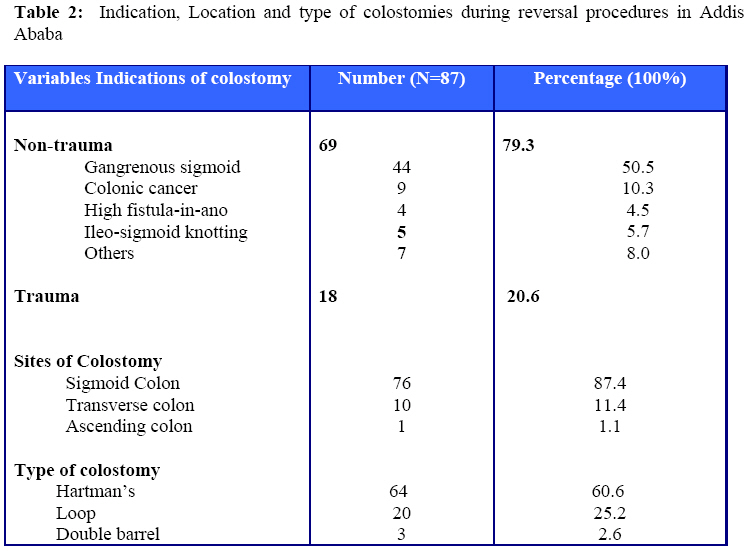
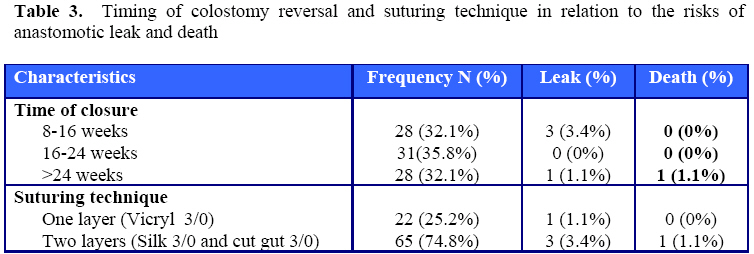
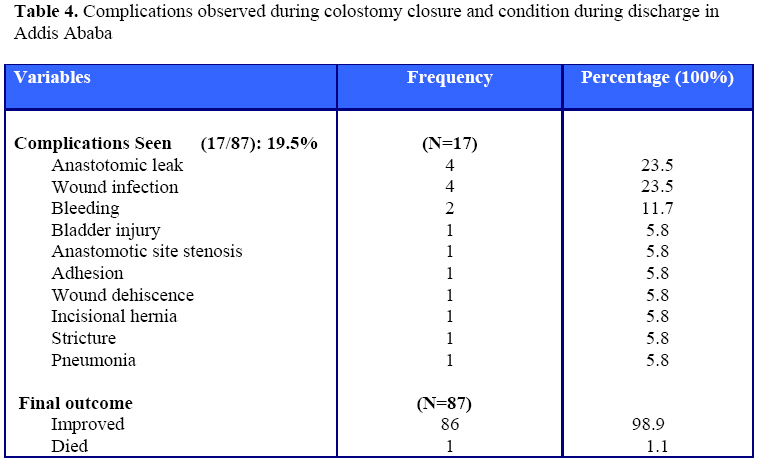
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 119-124 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts Department of surgery, Addis Ababa University, Faculty of Medicine. Code Number: js08045 Background: Colostomy creation and reversal procedures are common procedures, frequently performed by surgeons working in Ethiopia. Collected information is lacking concerning the outcome of colostomy reversal procedures in the country. Introduction Surgeons used to perform colostomies as life saving procedures since a long time. Majority of these procedures are performed in the settings of complicated sigmoid volvulus, colonic injuries and obstructing or perforated colonic cancers1,2. The classical Hartman’s procedure described by Henri Hartmann more than 80 years ago was an operation for resection of a cancer in the distal sigmoid and upper rectum and the formation of a permanent sigmoid colostomy3. Subsequent surgeons have recognized the value of the procedure in acute left-sided colonic disease, such as a gangrenous sigmoid Volvulus, colonic trauma and complicated diverticular disease4.5, where the colostomy could be reversed at a later stage when the patient had recovered6. Reversal of a Hartmann’s procedure is often considered a major undertaking. Operative mortality rates as high as 10%, morbidity rates of 30%-40% and anastomotic leakage rates of 15% have been reported7. It is also reported that almost half of the patients who have undergone a Hartmann’s procedure do not have their colostomy closed1. Though colostomy creations and reversals are frequently performed by Ethiopian surgeons, collected information is lacking concerning the timing of colostomy reversal, the complications of colostomy closure and final outcome of patients who underwent colostomy reversal procedure. Therefore, this review is intended to present the patterns of patients who underwent colostomy reversal, the timing of reversal, the frequently witnessed complications and the postoperative outcomes of patients operated upon for colostomy reversal procedure at the Tikur Anbessa and Saint Paul’s hospital in Addis Ababa, Ethiopia over a three year period. Patients and Methods The study was a retrospective analysis of patients who underwent colostomy reversal procedure from September 2004- 2007 (Over a three year period) at the two teaching university hospitals in Addis Ababa Ethiopia, namely the Tikur Anbessa Hospital (TAH) and the Saint Paul’s Hospital (SPH). Data was collected from the patients’ case records by using structured questionnaires. The variables included were the Socio-demographic profiles of the patients, the types and indications of colostomy, timing of colostomy closure, suture techniques, the frequently seen complications during the reversal procedure and the outcome of patients. Statistical software EP-INFO-Ver. 2002 was utilized for data analysis. Routinely before the procedure, all patients went through bowel preparation, which included colonic lavage through the colostomy and through the anus, laxatives, fluid diet for few days before the surgery and preoperative oral antibiotics. All surgeries were done under general anesthesia. For closure of Hartmann’s and double barrel colostomies, the previous incision was re-opened, while loop colostomies were reversed by in-situ mobilization. Results A total of 87 patients were studied. The majority of patients were males 70 (82.8%); the male to female ratio was 4.1:1 and in their 4th and 5th decades of life 37(42.5%). Most, 55(63.2%) came to the hospitals from a considerable distance from Addis Ababa (See Table 1). During the study period, there were 155 patients who were operated on for the creation of colostomies. The three most common indications of colostomy creation were Gangrenous sigmoid Volvulus in 56 (36.1%), Colonic cancer in 45(29%) and Colonic trauma in 28 (18.1%). The classical Hartman’s and loop colostomy were the most common types of colostomies performed in 94 (60.6%) and 39(25.2%) of the patients respectively. However, from these 155 patients, only 122 patients were discharged with a functioning colostomy, and only 87 (70.1%) of those discharged had their colostomy reversed. Table 2 shows the disease patterns that required colostomy creation and reversal. These included (from the 122 patients discharged with a functioning colostomy) 44/49 (89.7%) of the gangrenous sigmoid volvulus cases, 18/22(81.8%) of the colonic trauma cases and 9/32 (28.1%) of the colonic cancer patients. Seventy-six (87.4%) of the colostomies were situated in the sigmoid colon, 10(11.4%) in the transverse colon and 1(1.1%) was right-sided. Hartmann’s colostomy was the most common type in 64 (73.5%), followed by loop colostomy in 20 (23%) and double barrel 3(3.5%) The interval from the colostomy creation to colostomy closure varied from 8 weeks (2 months) to 72 weeks (18 months) with a mean interval of 28.2 weeks (6.6 months) and a SD of 3.5 months. The mean post-operative hospital stay was 11.9 days. Most, 71(81.6%) of the procedures, were performed by consultant surgeons; 16(18.4%) were done by residents under training. Reversal of colostomy was frequently performed by using the two layered hand-sewn method in 72 (82.8%) patients and one-layer hand-sewn closure in 15 (17.2%). Primary closure of all colostomy site wounds after thorough lavage was the choice of colostomy site treatment (Table 3). The overall incidence of complication was 17(19.5 %). Complications seen in patients with trauma were 4/18(22.2%) and in patients without trauma, it was 13/69(18.8%). Wound infection developed in 4(4.6 %) and anastomotic leakage occurred in 4(4.6 %). One patient who underwent sigmoid colostomy reversal created initially for gangrenous sigmoid volvulus died after anastomotic leak, making the overall mortality rate 1.1% (Table 4). More complications occurred during Hartmann’s colostomy reversals 13/17(76.5%), followed by 3/17(17.6 %) for loop colostomies and 1/17(5.8%) for double barrel colostomies. Whether the procedure was done by a consultant or a surgeon under training, there was no statistically significant difference. The morbidity of left sided colostomy reversal was 15/82 (18.3%) and 1/5(20 %) for transverse colostomies. The morbidity rate for reversal within 16 weeks (4 months) of its creation was 3/28 (10.7%) for those within 16 to 24 weeks, 0/28(0%); and for those after 24 weeks, 1/29(3.4%). Discussion In the study period, colostomy reversal procedures accounted for 87/7888(1.1 %) of all procedures done in the two hospitals. This review revealed male predominance over female and almost similar distribution of age groups. More colostomy closures were performed for patients from outside of Addis Ababa probably from rural communities. Similar to some authors, this review revealed statistically significant proportion (P<0.001) of colostomy closures performed for pathologies on the sigmoid colon1,2. Gangrenous sigmoid Volvulus followed by Colonic cancer were most frequently performed indications for colostomy closure1,2. Although up to half of patients who have undergone Hartmann’s procedure might not have their colostomy closed1, the rate of colostomy closure (70%) in this series was similar to most authors including colostomy closure in children1,13. In our series, we have demonstrated that a significant proportion (71.9%) of patients with colonic carcinoma fail to have their colostomy reversed. These can be explained by the fact that the main indication of colostomy in these patients might be for permanent colostomy intended for simple fecal diversion in the setting of advanced diseases, or following abdomino-perineal resection or some of the potential candidate of closure might have died with their colostomy. In agreement with some reports, most of the colostomies and colostomy closures were in the left colon8. Similarly, in accordance with J. Graham Williams, the classical Hartman’s colostomy reversal was the most common type of procedure, followed by loop colostomy closure4. Long interval, 8 weeks to 72 weeks, with a mean interval of 28.2 weeks from the colostomy creation to closure was the out come of this study compared to mean interval of 12.2 weeks by some authors7. In general, our study and that of Wani SA revealed the optimal timing of closure varies from patient to patient, but report by Cha SH concluded that closure within 6 weeks of the initial operation significantly increased the morbidity9, which is in line with our observation of 10.7% morbidity in those who underwent early reversal. Operative mortality rates as high as 10%, morbidity rates of 30%-40% and anastomotic leakage rates of 15% have been reported7. In our series, we have seen that the overall incidence of complication 17 (19.5 %) was lower than that of Cha SH who reported 25% morbidity rate. Anastomotic leakage occurred less frequently or similar to some authors7-9. The incidence of complications in our patients with trauma (22.2 %) was found to be significantly lower than those reported by Cha SH who reported 44.4%9. In our non-trauma patients, the incidence of complication of 18.8% is found comparable to 15.8% of Cha SH. The higher rates of morbidity of Hartmann’s colostomy reversal than for loop colostomy and for colostomy on left side than transverse colostomies was in agreement to other similar studies8,9 There was no statistically significant difference in the outcome or complication rates of colostomy reversal whether the surgery was done by a consultant surgeon or whether two layered or one layered suture technique was used. Therefore, in our setting one layered-interrupted closure method with absorbable suture such as 2/0 Vicryl can be practiced safely. The mean post-operative hospital stay was 13.9 days, which is significantly lower than the report by Wani SA (20 days). Although, primary closure of all colostomy site wounds was the choice of wound management in our cases, there are few authors who are advocates of delayed primary or secondary skin closure, given the significant risk of wound infection10,11. Conclusion We have found out that colostomy reversal is a low morbidity procedure in our setting and the optimal timing of closure varies from patient to patient. Since it is a relatively common procedure, all surgeons including surgeons under-training should be well versed with it. However, it appears that delayed reversal seems more advantageous and safer as compared to early reversal procedures. Colostomies on the left side are associated with a higher morbidity rate than transverse colostomies or colostomies on the right side. Acknowledgment We would like to acknowledge all surgeons, residents interns and the ward staff involved in the care of these patients. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08045t3.jpg] [js08045t1.jpg] [js08045t4.jpg] [js08045t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}