 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
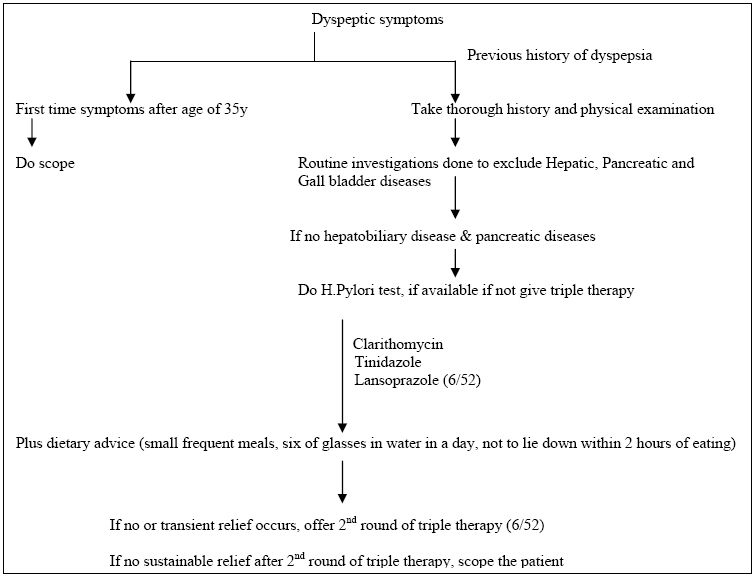
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 142-149 Gastric Cancer Diagnosis and Treatment guidelines 2008: Uganda Cancer Working Group M. Galukande M, A. Luwaga2, J. Jombwe1, J. Fualal1, J. Kigula-Mugamba2, A. Kanyike2, A. Gakwaya1 1Surgery Department, Faculty of Medicine, Makerere University2Radiotherapy department, Mulago Hospital, Kampala, Uganda Code Number: js08048 In Uganda most cancers to the exception of bladder and penis are increasing in incidence. The incidence of cancer of stomach is 5.6/100,000 from 0.8/100,000 in the 1960s a seven fold increase.The purpose of this guideline document is to highlight the salient points in gastric cancer diagnosis and treatment in the Ugandan context. It doesn’t only outline what is practical and efficacious but also our aspirations of practice as resources committed to the whole area of Oncological care services improve in the country. The primary and secondary prevention strategies are outlined. The multistage process of gastric oncogenesis is discussed in relation to the scientific basis of diagnostic and screening procedures. The treatment modalities including surgery radiotherapy and chemotherapy are discussed. A prognostication scale is included. Traditionally gastric cancer presents late and with a poor prognosis. The greatest strategy we have for management is in primary and secondary prevention. However a better understanding of how it arises (risk factors) will be important in informing prevention and treatment strategies. The Uganda cancer-working group intends that this information is disseminated to wider readership in the region as part of the strategy of improving Oncological care service in the region. Introduction This document contains information about the epidemiology, presentation, investigations, and treatment for early and late disease complications of treatment as well as prognosis. Whereas over the past several decades gastric cancer as dropped in incidence globally1, in Uganda most including gastric cancers have increased in incidence to the exception of bladder and penis cancer. This coincides with marked social and lifestyle changes and with the emergence of AIDS epidemic. The incidence of cancer of stomach is 5.6/100,000 from 0.8/100,000 in the 1960’s, a seven-fold increase2. Gastric cancer traditionally carries a poor prognosis because it presents at an advanced stage of the disease. If diagnosed at an early stage, it is a curable disease. Strategies to improve outcomes are: to promote primary prevention strategies of eradication of Helicobacter Pylori in endemic areas with high incidence of gastric cancer, encourage diet rich in vitamin C, fresh fruits and green leafy vegetables3. Early detection by screening high-risk individuals or groups, improvement of treatment and improving of our biological understanding of gastric carcinogenesis1. The highest risk is in individuals with hypochlorhydria or achlorhydria with extensive atrophy4. Gastric cancer is believed to arise via a multistage process that includes chronic gastritis or and gastric atrophy usually with Intestinal metaplasia and finally dysplasia5. Because the development of gastric carcinoma is slow and unpredictable, investigators have searched for premalignant markers of increased risk for gastric cancer. Intestinal metaplasia sub-typed as III is considered an ominous precursor lesion for the intestinal form of gastric cancer as indicated in the preliminary data from a prospective study from three centres6. The Uganda Cancer Working group is mandated by the Ministry of Health to guide clinical care, standardise Oncology practice and promote awareness of important Oncological conditions. These guidelines serve as a learning resource for health workers as well as serving the purpose of documentation of care in a resource-limited environment. Clinical presentation7, 8, 9, 10, 11 Gastric cancer is difficult to diagnose early because there is usually a time lag between the onset of growth and the appearance of symptoms. These include but not limited to gastric distension, easy satiety, vomiting, anorexia, weight loss, anaemia, haematemesis, tiredness and weakness. Epigastric pain with lack of periodicity and non-responsiveness to treatment is a late feature. The patients may be conveniently grouped into five categories. Group I. New dyspepsia after 40 years; with indigestion and no past history suggestive of PUD. The above can be rearranged into 2 categories: Early symptoms: Group 1 and Late symptoms: Group II – V. For purposes of ‘catching’ cancer of the stomach early, we consider new dyspepsia after the age of 40 and patients (irrespective) of age presenting with longstanding history of dyspepsia to be investigated for cancer of the stomach. (UGI endoscopy or barium contrast Studies. Proposed Algorithm for managing Dyspepsia at the district hospital (Fig 1) Screening and Diagnosis12,13,14,15,16 Routine screening for gastric cancer is currently not practiced in Uganda. However, the following screening procedures may be carried out in some specialized clinics for asymptomatic patients seeking medical check ups.
Diagnosis Upper Gastrointestinal Endoscopy This investigation facility provides direct visualization of gastric mucosa and allows biopsy of any suspicious areas, evaluation of anatomical extent of gross disease and assists in planning therapy. Abnormalities that indicate possible malignancy include hyperaemia, mucosal irregularity, ulceration and/ or a frank mass. A Double Contrast Barium meal This is a procedure in which radiographs of the oesophagus, stomach and duodenum are taken after ingestion of barium sulphate and a gas-forming agent by the patient. Barium meals are useful in the diagnosis of structural and motility abnormalities. Gastric carcinoma usually appears as a polyploidy, ulcerative or infiltrative lesion. However many tumours have mixed morphological features so that considerable overlap exists on the radiographs. The infiltrative carcinomas cause narrowing of the lumen and rigidity of the stomach, producing a linitis plastica or leather bottle appearance. Staging Investigations Patients require a full blood count, urea and electrolytes, liver function tests liver ultrasound and baseline chest x-ray prior to surgery. The routine use of CT scan, skeletal survey and skeletal scintigraphy (Bone scans) in asymptomatic patient has very low yield and does not improve survival or quality of life. Pathology The common histological subtypes are:
Minimum information required from biopsy specimens is:
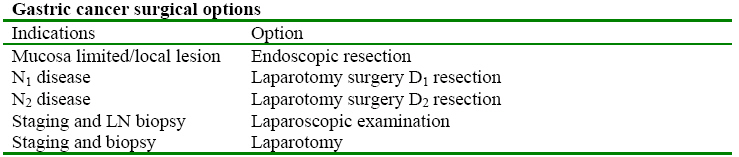
For endoscopic biopsies only the third to the fifty bullets apply. Surgery3,7,12,17 Surgery is the only treatment that has an effect on the natural history of gastric cancer, however this benefit is limited to patients who present with early and perhaps local disease. Most of the patients we see in Uganda present in the late stages. Surgery is the best method of secondary prevention this applies to patients with localised disease, including those with lesions confined to the stomach wall and those with local lymph node involvement. The lymph nodes are classified in relation to the primary; those with 3 cm of the primary are classified as N1, the second tier of nodes (N2) vary according to location of the primary, but are essentially those that can be removed by resection, the more distant nodes are classified as N3. Surgical resection is described as D1, if the N1 nodes are excised and D2 if both N1 and N2 nodes are excised. Role of surgery Diagnosis: this may be done by endoscopy examination or at an exploratory laparotomy. Gastric cancer surgical options (Table 1) Types of Surgery D1 resection -surgical resection (partial or total gastrectomy)
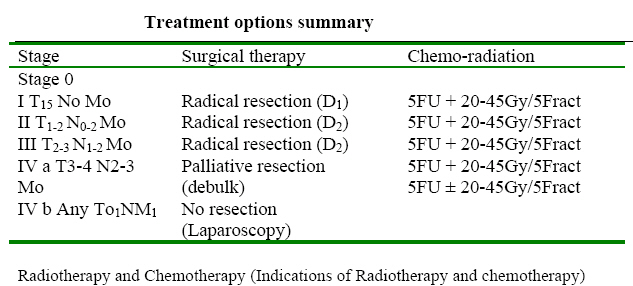
with N1 Node dissection The right gastroepiploic artery is divided as it’s ongoing from the gastroduodenal artery. The right gastric artery is divided on the lesser curve. The lesser momentum is taken off the liver up to the hiatus. The pylorus is divided allowing the entire stomach to be lifted the lymph node dissection starts up by removing the nodes from the gastroduodenal artery and extending this up to its origin on the common hepatic artery to the porta hepatis. The lymph nodes are then cleared medially along the common hepatic artery to its origin from the celiac axis. The nodes are cleared from around the celiac axis and out along the splenic artery to the splenic helium; this is facilitated by mobilising the spleen and distal pancreas. When all these lymph nodes have been cleared, the stomach is removed. For lesions of the middle and upper third of the stomach, a total gastrectomy is appropriate for lesions of the antrum, a high partial gastrectomy leaving the spleen is appropriate (the lymph nodes at the splenic helium are N3 nodes for antral lesions and this type of surgery should not be considered if they are involved.A total gastrectomy should be reconstructed as a Roux en Y with a 60cm Roux to prevent bile reflux. A partial gastrectomy is best reconstructed as a polya type of gastrectomy. Treatment options summary (Table 2) External beam/radiation is administered with concomitant (5FU)-based chemotherapy. This is indicated in;
Radiation technique The treatment portals used were developed from studies looking at the patterns of failure in preoperative series of gastric cancer19. However, these are modified on individual basis and also following the guidelines for defining clinical target volume for post-operative irradiation20. Patients in general should have a field covering the remaining part of the stomach, surgical margins and clinical positive nodes. If greater than 10 – 15 lymph nodes are pathologically negative, then lymph nodes involvement in the treatment field is optional21. The 3-Dimensional Conformal Radiation Therapy (3-DCRT) with more than 2 fields reduces the toxicity to critical structures, but only accurate if the reconstruction of tumour from preoperative imaging is possible and intra operative tumour bed clips are used22. Parallel-opposed Anterior Posterior/ Posterior Anterior (AP/PA) fields are the practical arrangement in Uganda. In general, the average field used is 15cm x 15 cm treating with 1.8 – 2 Gy per fraction up to total 45 Gy23. The lead blocks are usually used where necessary to limit the dose to the above structures within normal limits during treatment. However its important to include celiac axis T12 – L1 and portal hepatic lymph nodes that are only well covered with field extending 2cm to the right of T11 – L124. Chemotherapy The 5FU-based chemotherapy is standard treatment in gastric cancer. 5FU has been shown to sensitise the cells to radiotherapy (5FU is a pyramidine analog which blocks thymidylate synthatase thereby blocking DNA synthesis). The 5FU has a short half-life (20 minutes) and therefore is better given as a continuous infusion during radiotherapy. However, it is usually given as a bolus with Leucovorin (Folinic acid) which potentates its activity. Therefore, all patients with high-risk cancer of the stomach are given 5-FU/leucovorin usually after the 4th post operative week (MacDonald 2001), the Full Blood Count /Liver Function Tests/Renal Function Tests are done and should be in normal range before chemotherapy, patients with febrile condition should be treated until the temperature is normal before starting chemotherapy, dose may be reduced if on subsequent blood results, LFTs are compromised. Pre and post medication with anti-emetics is important in order to reduce the side effects of the chemotherapy. Other chemotherapeutic agents like capecitabine (oral 5-FU), Oxaleplatin, Irinotican can be used in combination or as single agents especially in the metastatic state. Appendix IV gives the chemotherapy dosage details. Side Effects of chemotherapy Combined chemo-radiotherapy would give more side effects than either. Common side effects are nausea, vomiting and diarrhoea. Palmer-foot syndrome is rare. If the side effects are severe or intolerable chemotherapy or radiotherapy or both should be withheld until improvement, usually the haematological recovery occurs in 21days. Haemopoietic growth factors may be useful in cases of low white cell counts to prevent severe infection. Palliative Radiotherapy25 This provides control of local symptoms. We anticipate that 50% - 75% of patients would have symptomatic relief of ; pain, gastric out-let obstruction relief, cessation of bleeding and biliary obstruction relief. The palliative benefit is more the smaller the tumour bulk is. It also works well if patient have a good performance status score. The best palliation is with concomitant 5FU. The duration of palliation varies from 4-18months23. Radiation dose: 20Gy divided in 5 fractions to 45Gy at 1.8Gy per fraction with or without 5-FU based chemotherapy, usually 6 cycles is recommended. Prognostication26, 27, 28, 29 Pre malignant conditions The following conditions are considered as pre-malignant; gastric atrophy, atrophic gastritis, intestinal metaplasia and severe H.Pylori infection and they should be handled as suggested below:
Prognostication for early and late disease Early lesions: Anticipate cure (see 5 year survival below) 5 year Survival rates
Conclusion Gastric Cancer incidence is on the increase in Uganda. The critical strategies are to understand the reasons why, so as to inform locally applicable interventional strategies including prevention. The other important strategy is to standardize clinical approach to diagnosis and treatment as an endeavour for optimal utilization of available and limited resources as well as impact on outcomes. References
© 2008 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js08048t2.jpg] [js08048t1.jpg] [js08048f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}