 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
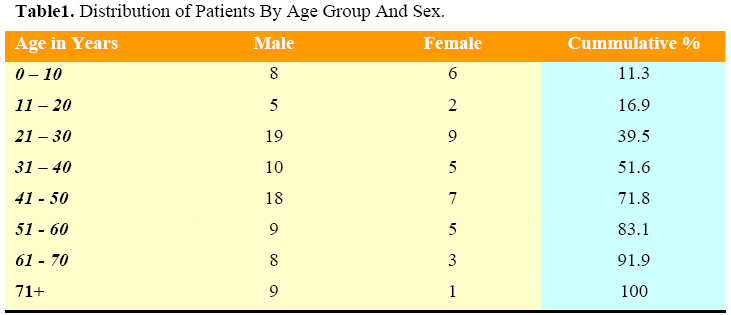
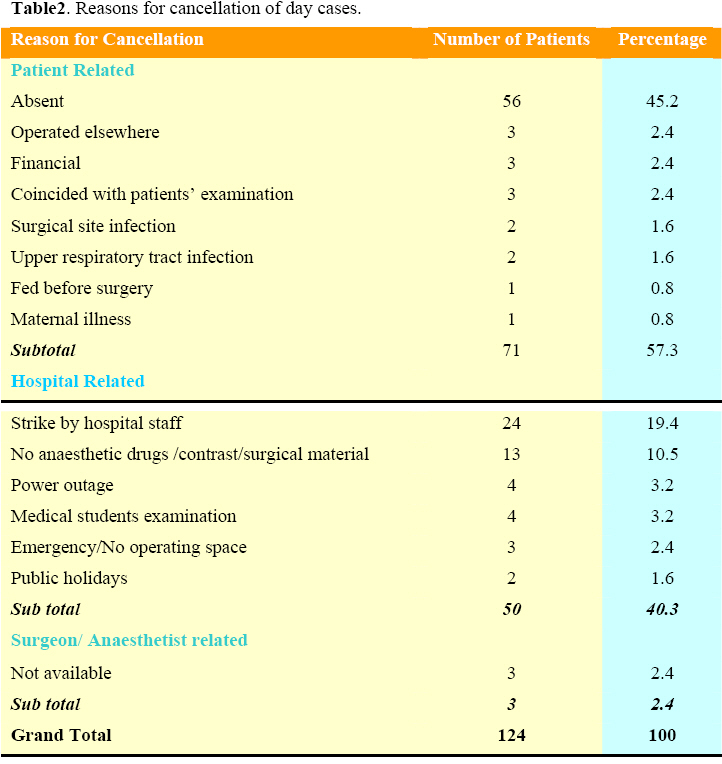
East and Central African Journal of Surgery, Vol. 13, No. 2, September, 2008, pp. 150-153 An Audit of Day Case Cancellations In A Nigerian Tertiary Hospital Based Day Case Unit E.O. Ojo, C.H. Ihezue Departments of Surgery; Jos University Teaching Hospital, Jos, Nigeria Code Number: js08049 Background: The concept of day case surgery puts into efficient utilisation scarce resources to derive numerous social and economic benefits. Frequent cancellation however erodes these gains and therefore serves as a way of assessing the efficient utilisation of day case resources including the factors responsible for under utilisation. The objective of this study was to assess the extent and reasons for day case cancellations and consequently the degree of its efficient utilization. Introduction Surgical cancellation has been likened to an adverse event that needs to be monitored routinely in the hospital because of its implications on the health systems and the patients1. It is a major cause of inefficient utilisation of scarce resources including that of the operating room and valuable manpower. Last minute cancellation constitutes a waste of time for the surgeon and other staff that might gather for an agreed schedule. Cancellation is stressful and demanding on patients and their employers in terms of loss of working days and causes disruption to daily life which could be very emotionally distressing to the patients2,3. It equally robs other patients on the long waiting list of timely opportunity of getting their operation done. Frequent day case cancellations in a day case setting therefore, whittle down the potential benefits of the huge investment in establishing such facility through suboptimal utilisation. Patients and Methods This was a prospective study done in the Department of Surgery, of the Jos University Teaching Hospital, Jos from January to December 2004. The study is a follow up to a six month assessment of cancelled day cases in three units of the Department four years earlier in the same institution4. All the patients were evaluated and counseled for surgery at the out patient clinic with informed consent obtained. They all had base line haemoglobin and urinalysis done and those for general anaesthesia also had electrolyte, urea and hemoglobin genotype. Other investigations were dictated by the diagnosis. The categories of patients booked for day cases included: patients willing to be operated as day cases, those with a responsible adult to accompany them and look after them at home, conducive home environment, haemoglobin of at least 10gm/dl or packed cell volume of 30%, patients with the American Society of Anaesthesiology grades one or two, operations not lasting more than one and half hours, availability of transport to a health facility in the event of a complication occurring at home that needed urgent attention. Excluded were patients on immunosuppressant or steroid therapy, evidence of bleeding diatheses, those residing beyond thirty kilometer radius from the hospital and all emergencies. They were scheduled for various operations under local, regional or general anaesthesia. Due to lack of a dedicated unit, day cases were carried out first in the morning using the same theatre with in-patients and were then admitted into day case ward before proceeding with inpatients’ operation. Patients who consented to day case surgery but whose procedures were cancelled on the day of surgery for any reasons form the basis of this study. Data were obtained in a proforma for analysis and this included the patients’ biodata, the scheduled procedures and the reasons for the day case cancellations. Analysis was done using Epi Info 2004 version 3.3.2 Results A total of 435 patients were planned for day case surgery by the seven units of the Department of Surgery of the Jos University Teaching Hospital, Jos during the period of the study. Of these, 311 patients were operated as day cases while the remaining 124 patients’ procedures were cancelled for various reasons giving a cancellation rate of 28.5%. A total of 1024 elective patients were operated during this period resulting in a day case surgery rate of 30.4%. The age of the patients whose procedures were cancelled ranged from two weeks to 85years (Mean 39.1±22.1SD). There were 86 (69.4%) males and 38(30.6%) females with a ratio of 2.3:1(Table 1). They were scheduled mainly for cystoscopy in 47 (37.9%) patients, hernia repair in 20 (16.1%) patients, lumpectomy in 20 (16.1%) patients, upper/ lower gastrointestinal endoscopy in 11(8.9%) patients and the rest were booked for revision of scar, biopsies, anal/urethral dilatation, vasography etc. The reasons for day case cancellations were patient related in (57.3%), hospital related in (40.3%) and surgeon or anaesthetist related in (2.4%) as shown in Table 2. Discussion A day case cancellation rate of 28.5% is high as over a quarter of the patients scheduled for surgery were eventually cancelled. The value has almost tripled the 10% reported by Macarthur et al5 and higher than 19.3% cancellation found in Lagos6. This reflects a high degree of wastages in our day case practices. The value is however less than the 36.4% previously found in the same centre by Ramyil et al4. This is because while there has been reduction in surgeon and patient related factors there has also been coincidental increase in hospital related causes thereby still leaving us with a high cancellation rate. Patient related causes accounted for 57.3%. This is lower than 74.4%4 previously reported but similar to the of 62% of Bode et al6. Majority of these patients failed to turn up for their procedures on the day of surgery with no apparent reasons. Patient education during out patient surgical preparation on the consequences of defaulting must be intensified and sustained to further reduce this. Patients should also be seen in the out patient clinic as close to the day of operation as possible to further ascertain their commitment and readiness, thereby reducing last minute cancellations. The impact of such late out-patient consultation may then be subsequently evaluated against an early one as done for day case anaesthesia7. While pre-operative community nurse visits as employed elsewhere8 may not be immediately feasible in developing countries due to staff constraints, the increasing availability of mobile phone networks may ensure the usage of telephone calls to reduce cancellations9.Three cases (2.4%) were cancelled for lack of funds; this scenario could be eliminated by ensuring that all patients are financially ready before they are enlisted for operation since our day cases are elective patients. This study found a substantial increase in hospital related cancellations with a rate of 40.3%. It has tripled the 13.3%4 previously documented and is also higher than 28%6 previously found in Lagos. These causes are quite preventable. Various strikes were embarked upon by the hospital staff to demand for better welfare/working conditions and improvement in dwindling infrastructure. This accounted for about half (48%) of the hospital related causes and reflects the extent of neglect and infrastructural decay in our hospitals. Since day case practices in this part of the world are essentially hospitals based units, this trend must be curtailed by the hospital management and the health ministries by adopting the necessary strategies to stem hospital related wastages that are on the increase10. Frequent power failure and lack of surgical/theatre materials are not insuperable with a good focus. Lack of operating space and interruption of day case lists by emergencies are surmountable with proper planning and dedicated day case units. Three patients had their procedures done elsewhere due to delay in carrying out their procedures. Although they represent only 2.4% of the cancellations, their case is instructional that we must minimize delays and reduce our waiting time for surgery as much as possible. This can be achieved by garnering resources from maximal utilisation of the available facilities towards further expansion for efficient services11. Medical students’ examinations and other programmes should be planned ahead in adequate time to forestall interference with the operation list. Established public holidays should be looked for and marked out in the day case booking registers from the beginning of the year to reduce the incidence of booking patients against public holidays. In conclusion, we found a high cancellation rate from preventable causes with an increasing hospital related component in this study. This constitutes a bane to a qualitative, efficient and rapid day case expansion in a continent where day case practice is predominantly hospital based with non existent freestanding facilities if it is unchecked. There is every need to forestall further wastages by focusing attention on hospital welfare and general infrastructural developments complemented by better planning of day cases with refined pre operative patient counselling and booking. Establishment of dedicated day case units will also go a long way in providing more efficient day case services. References
© 2008 East and Central African Journal of Surgery |

{kind=link}
{kind=link}