 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
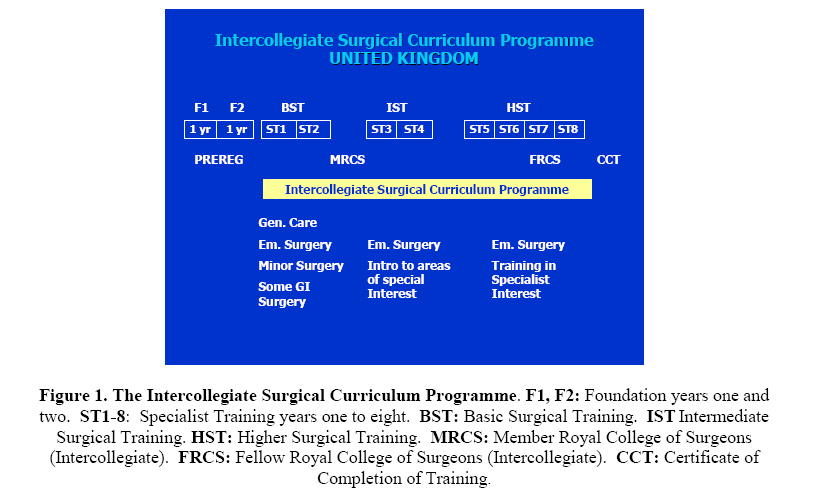
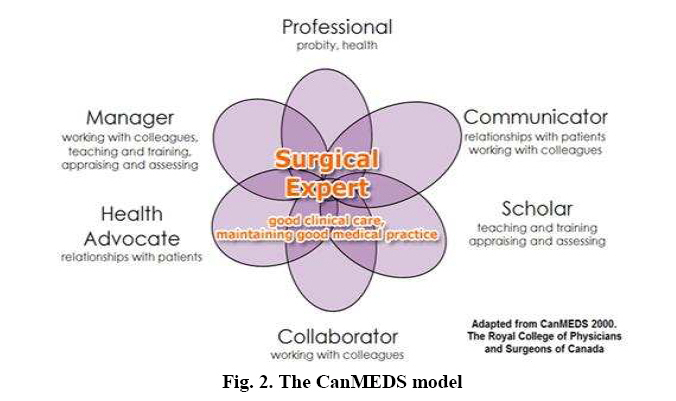
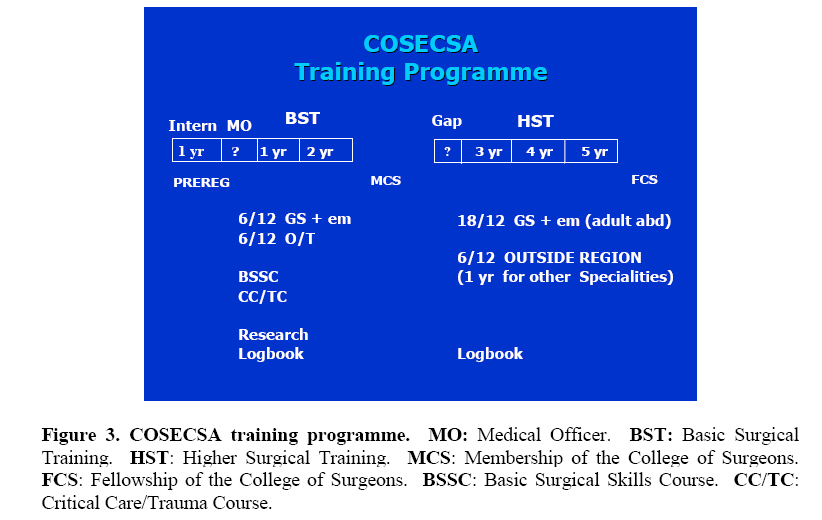
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 1-12 The Rahima Dawood Memorial Lecture – Maputo, Mozambique 2008 Surgical Education & Training in the COSECSA Region Robert Lane Code Number: js09001 INTRODUCTION I should first like to thank the Trustees of the Rahima Dawood Foundation for inviting me to be the Travelling Fellow this year and in particular to Dr Yusuf Kodwavwala who named this Foundation after his parents, Rahima and Dawood in 1987. It is indeed a very great honour and I tread hesitatingly in the footsteps of many illustrious former Fellows. I have had the good fortune to visit six countries within the Region and I take this opportunity to thank my hosts for their enormous kindness and hospitality. BACKGROUND The most important remit of COSECSA is to oversee surgical education and training in the Region. I intend in this lecture to discuss the background as to why this is so important, to report on the current situation in the UK and in the Region (mainly with reference to general surgery), to identify certain problem areas and to put forward some possible solutions and finally to discuss what I perceive to be the future of COSECSA. Why are we discussing this subject? Forty-six out of the fifty-three countries in Africa are faced with a critical shortage of health workers. It is estimated that the number needs to increase by 139% to address health needs in Africa and that translates into one million more health workers. Africa has 24% of the global health burden but only 3% of the global health workforce whereas the United States of America has 10% of the global health burden and 37% of the global health work force1 . These stark facts put the situation into perspective. Nobody can doubt that there is a problem that needs addressing. It is no surprise, therefore, that four out of the eight Millennium Development Goals (MDG’s) are health related. CURRENT SITUATION IN THE UK The situation in the UK has changed so many times in recent years that I can only report on my perception as to where we are now. The original concept was to reduce the length of training which was perceived to be too long and inequitable when compared to other countries within the European Community. However, whilst this matter was being addressed other confounding issues relating to UK immigration, the European Working Time Directive2 and a changing NHS environment intervened and this is partly why it has been so difficult to re-design surgical education and training. Two Foundation years (F1, F2) are undertaken post-qualification prior to registration and during this period the graduates rotate through the major specialities of Medicine. (Fig.1). The training pathway in the speciality of General Surgery has been laid down by the Intercollegiate Surgical Curriculum Programme3 (ISCP). The syllabus supports a curriculum that is divided into three Stages which together form the training continuum through to a Certificate of Completion of Training (CCT) within the speciality. The curriculum is competency based and progression is dependent upon the acquisition of specific goals set for each Stage which are considered as annual periods as this coincides with the annual assessment process. The first Stage, Basic Surgical Training, requires competitive entry and takes two years (ST1, ST2). This Stage includes general care of the surgical patient, minor operative procedures, some gastro-intestinal and emergency surgery. A satisfactory conclusion of basic surgical training includes passing the Intercollegiate MRCS examination following which there is competitive entry into the second Stage, Intermediate Surgical Training, which takes two years (ST3, ST4). This stage includes a short introduction to the areas of special interest within general surgery and a continuation of emergency surgery. If the Annual Reviews are satisfactory there is then seamless progression into the third Stage, Higher Surgical Training, which takes four years (ST5-ST8). This stage includes training in an area of special interest and further general and emergency surgery. Towards the end of this period the trainee will sit the Intercollegiate FRCS examination which will, if successful, lead to a CCT provided that annual reviews are satisfactory. Emphasis needs to be made that this training is not ‘time’ based but ‘competency’ based. It includes workplace based assessments covering skills, knowledge, behaviour and attitudes, a comprehensive log book of procedures including outcomes, the passing of examinations and an annual learning agreement between the trainee and an assigned educational supervisor whose report at the end of the year will influence the Annual Review of Competence Progression (ARCP) undertaken by a Regional panel who report to the Post Graduate Dean. Despite the original concept to reduce the length of surgical training in the UK, it remains as long as it was before! The reason for this relates to the confounding factors mentioned above and, in particular, the European Working Time Directive which stipulates that from 1st August 2009 no trainee will work more than an average of 48 hours per week. For this reason the Surgical Royal Colleges and the Speciality Associations, in particular, objected to any shortening of training. The Canadian Medical Education Directions for Specialists (CanMEDS)4 model was chosen as a basis for the ISCP as it identifies seven key roles of a doctor which encompass the following domains:-Knowledge, Judgement, Technique and Professionalism. The seven key roles interact with each other combining to produce the surgical expert. (Fig.2) It is evident that being a good surgeon is much more than simply being a good technician. It may be felt that these roles are self-evident, as indeed they are, and I am sure they will resonate with each and every member of the audience. The vast majority of complaints in the UK arise through a lack of communication. Team working is becoming essential with increasing specialisation. Health advocacy, on behalf of patients, was influential in getting a decision concerning anti-cancer drugs reversed by the National Institute for Clinical Excellence (NICE) in the UK who initially rejected them mainly on grounds of cost effectiveness even though these drugs were available elsewhere in Europe including Scotland. Management of resources is very important and in the UK the Profession abrogated their responsibilities sometime ago and as a result have been marginalised by Government. Be warned! The Non-Technical Skills for Surgeons (NOTSS) handbook published by the University of Aberdeen (2006) is one example of a teaching aid to assist in learning some of these key roles. The role of leadership cannot be emphasised more strongly. Many of the hallmarks of good leadership are not difficult to apply and it is not surprising what trainees look for, and appreciate, in us their Consultants – punctuality, politeness, personal contact, taking an interest in their careers, their lives, their ups and downs and welcoming them as part of the Team. We often grossly underestimate the effect that we as Consultants have on our trainees and I am sure that if you all look back to the time when you were a surgical trainee you can remember vividly the chiefs you worked under who impressed you most …… and those who did not! We have to act as a role model by maintaining and adhering to appropriate standards of surgery and behaviour in our daily practice. CURRENT SITUATION IN THE COSECSA REGION A post-qualification internship for one year, apart from Malawi (18 months), Zambia and Zimbabwe (2 years), is followed by a variable number of years, average three, spent as a Medical Officer (MO) in the rural areas (Fig.3). Three countries, Malawi, Zambia and Zimbabwe allow trainees to enter straight onto a postgraduate programme without necessarily having to spend any time as a medical officer in the rural areas. However, elsewhere this period does allow for the consolidation of knowledge and experience within the generality of Medicine. There is the possibility of undertaking minor surgery but without any training there is the risk that the potential surgeon will learn bad habits which may persist. The length of time spent as an MO depends on how easy it is to get onto an MMed programme and, in some instances, how the fees and living expenses are going to be met. Once accepted training is seamless until a degree is obtained four or five years later depending upon the speciality. The programme involves rotation through the specialities and a dissertation which is compulsory. There is no great enthusiasm within the Region to sit the MCS examination apart from in Zambia and possibly Malawi. Twenty percent of interviewees intend to or have taken the exam. Those that register for the MCS will receive a syllabus and must satisfactorily complete two years of Basic Surgical training in recognised posts in approved centres in the Region which must include at least six months of general surgery involving emergencies and at least six months of orthopaedics and trauma. The remainder of the time may be spent in any surgical speciality including the above. Attendance at a Basic Surgical Skills course and a Critical Care or Trauma course is mandatory. Research is encouraged although not apparent during my visits. Trainees have to keep a log book which is critically assessed at the examination. The situation following satisfactory completion of the MMed plus or minus the MCS differs from country to country. In one there appears to be no formal specialist training in general surgery and trainees have to go abroad. In others there is either seamless training or competitive entry onto a specialist training programme which lasts for 1-3 years. Of those interviewed, 64% intend to take the FCS in their speciality of choice. Those that wish to register for the FCS examination in general surgery should normally have passed the MCS or an equivalent examination such as MMed of one of the constituent countries of the ECSA community. Candidates have to spend three years in recognised supervised training posts; one and a half years of which must be spent in a general surgical unit dealing mainly with adult abdominal surgery. The remainder of the time can be spent in units specialising in other branches of surgery provided these deal with emergencies on a regular basis. Six months of the three years may be spent outside the Region in a post that has been prospectively agreed with the Examination and Training Committee. This post must be in an elective unit. During the training period candidates must keep a log book to record their training experience which will be critically assessed at the examination. The aim of this training depends upon what sort of consultant we wish to produce – a generalist, a specialist or both. This question is linked with where they will work. The answer depends very much on the need for specialists, ie: how many need training in each speciality at any one time PROBLEM AREAS AND SUGGESTED SOLUTIONS Difficulty with recruitment and emigration is due to a long training, difficult examinations, poor remuneration and an increased risk of HIV/AIDS. In addition young graduates are lured away from Government hospitals into Public Health.5 In one year they can obtain a Master’s Degree and can then earn good salaries with NGO’s and have a high expectation of being sent on courses or training overseas and, of course, some never return. In my view this is not the way to act in a fragile health system such as we have in our Region where 1:22 women die in labour6 and over 60% of the population has no access to emergency drugs.7 I wonder how much money is being thrown at these problems. However, I am pleased to report that a new Code of Conduct for NGO’s has been drawn up to address this issue and has already been signed by more than 20 such organisations so hopefully this situation will not happen to the same extent in the future.8 However, a robust, seamless and attractive Regional training programme leading to a Speciality qualification such as the FCS, as opposed to a long disjointed one, is far more likely to attract trainees and keep them in country thereafter.9 There needs to be a curriculum and that for the MCS and the FCS in their various specialities is currently satisfactory but, like all curricula, needs regular evaluation. An educational supervisor is essential without which progress cannot be assessed. The programmes, whether for the MMed or the MCS/FCS, require regular tutorials, mortality and morbidity, pathology, radiology, journal club, and audit meetings. I appreciate that there is a capacity problem with regard to chairing these meetings for it may be that there is a dearth, for instance, of histopathologists or radiologists in some Teaching Hospitals but, at the end of the day, it is not beyond the ability of consultant surgeons themselves to cover those aspects of these subjects relevant to surgery. Postgraduate activity succeeds better if the trainees have some responsibility for running these meetings. Postgraduate training does place a burden upon trainers. All postgraduate students undertake a heavy service commitment but nonetheless the programme should take into account time for training and personal study. All trainees appreciate the need for consultants to do private practice in order to earn a decent living. However, it is in private hospitals where the vast majority of high-tech surgery is performed and trainees do need access to these modern techniques if for no other reason than they will be examined on them in the MCS and FCS. Resources in Government Hospitals are very variable and especially in operating theatres and radiology departments. This minimises the potential for training whereas in Private Hospitals facilities are immeasurably superior. This is a wasted opportunity and I suggest that more ways of rotating surgical trainees through the Private sector to at least allow them to see modern techniques, let alone assist in operations, should be explored. Orthopaedic surgeons are more receptive to this than general surgeons. I do not think it is necessarily a case of trainees wanting to get extra remuneration for attending in Private Hospitals; it is simply that they really want to see modern surgical techniques using instruments and equipment that are unavailable in the Government sector. In the majority of Teaching Hospitals the main complaint with regard to library facilities was of old books and old journals. Computers, in general, are in short supply and not readily available. When they are, access is unreliable and very slow due to the fact that Broadband is not widespread. Four Teaching Hospitals had access to the Ptolemy Project (www.ptolemy.ca) but only one had access to Distance Learning and that was in Lusaka who are piloting the Basic Electronic Surgical Training (BEST) course online for the Royal College of Surgeons in Ireland. All trainees in Lusaka thought this was excellent. One Teaching Hospital had no access to the internet, thus no access to Distance Learning and no involvement with the Ptolemy Project. Each Medical School/Teaching Hospital should insist on good library facilities which must include up to date textbooks and readily available internet access which should be fairly fast. A collection of surgical journals spanning the various sub-specialities should be available although many articles can now be accessed via the internet (PubMed., Medline, etc.) and to this end every Teaching Hospital should have access to the Ptolemy Project, especially to the ‘Surgery in Africa’ monthly reviews whose objective is to provide a self-directed online journal based course for surgical trainees who are taking the FCS. The aim of Distance learning is to acquire knowledge and there are a number of courses available online, in addition to the BEST course, such as The Surgical Training Education Programmes (STEP) (Foundation and Core) which are produced by the Royal College of Surgeons of England. Each course includes materials, passwords and a subscription to the Journal ‘Surgery’ and runs for 24 months involving 15 hours of study per week over 20 months. Both can be visited at the Royal College of Surgeons of England website (www.rsceng.ac.uk). The SELECT course produced by the Royal College of Surgeons of Edinburgh has now been superseded by the Edinburgh Surgical Sciences Qualification (ESSQ) which is produced jointly by the College and the University of Edinburgh. This again is a Distance Learning course requiring approximately 10 hours per week. One year’s subscription will produce a Certificate, two a Diploma and three a Masters Degree. (www.info@rcsed.ac.uk). Simulation in skills labs is required to develop surgical expertise. These skills labs/workshops are proving increasingly popular for it is possible to train a group of surgeons at the same time to the same standard and more quickly than otherwise. Six years ago the Association of Surgeons Great Britain & Ireland (ASGBI) was invited to run a number of Basic Surgical Skills courses in the Region since when Ethicon ( a Johnson & Johnson company) have sponsored eight Skills Centres across the Region for two years and resourced them for two courses per year for 12 participants each. ASGBI have now moved on to develop anastomosis, laparoscopic and other workshops. Initially I was somewhat against training Residents in laparoscopic techniques when they had no means to maintain their skills in Government hospitals thereafter. However, I have recently changed my mind because I believe that diagnostic laparoscopy, and by this I mean the ability to look inside the abdomen and take biopsies but no more, is a practical alternative to CT imaging which is not always readily available in Teaching Hospitals let alone rural ones. The one course that everybody seems to want is Training the Trainers course and the Royal College of Surgeons of Edinburgh were instrumental in introducing one to the Region in 2006. These aids to education and training are a good example of partnership between COSECSA and the Royal Colleges, Speciality Associations and Industry. For all intents and purposes, apart from undertaking a dissertation for the MMed, research opportunities are minimal due to a lack of time, funding and supervision. There is also limited access to laboratories, the internet (see above) and Government health statistics. Many trainees felt that a dissertation for the MMed added little to training and in general was a wasted opportunity. However, research is an important aspect of our Practice and is one of the seven roles of a surgeon in the CanMEDS model. It enables us to digest and evaluate evidence and to assess and appraise the literature. Furthermore, it develops an enquiring mind and allows indepth study. There are a number of courses on research methodology which include statistical analysis. I suggest that these should be mandatory during the early part of both the MMed and the MCS courses. There is enormous potential for research in the Region particularly with regard to gaining a better understanding of the local burden of surgical disease and the resources needed to deal adequately with it. However, in my travels I saw very little evidence of research. It may well be that it is taking place through Institutions and NGO’s from outside the Region. We know that infective agents such as HIV, tuberculosis and malaria all command enormous sums of money for research but this should not mean that we simply give up. We have to impress upon grant giving bodies that research into surgical disease is just as important in the long run and worth supporting. I was disappointed to learn that in four out of the six Teaching Hospitals audit was either totally inadequate or non-existent. Audit need not be complicated and need not cost much10 – sometimes just pencil and paper! Audit is also research and is an essential and valuable clinical and educational tool which should be mandatory for all surgical teams including trainees. Although audit in clinical practice was not very evident, a number of dissertations for the MMed were audit based which was commendable. However, the real reason for lack of audit may have been related to the perceived cost rather than choice. Research and audit must adopt a higher profile in the training programmes in future. Again, it was disappointing that two Teaching Hospitals had no trainee assessment bar log books which were simply signed by the consultant without any discussion. In one Teaching Hospital they had no log books at all, as there was no supervision and operations could not be verified because the majority was emergencies done by trainees on their own! In the three remaining Teaching Hospitals log books were kept and there was useful discussion prior to consultants signing them. In two Teaching Hospitals there was regular assessment but in the others there was really no meaningful attempt to assess the trainees’ progress. Assessment and feedback are essential in a modern day training programme and I have outlined the methods used in the UK which I commend to you. It is important for the trainee to know whether he/she is progressing satisfactorily. Feedback is a two-way process. It is important that the Department of Surgery knows that their programme of training is satisfactory and also to be enlightened as to areas where perhaps improvement could be made. Again I emphasise that training must be ‘competency’ based and not ‘time’ based. As the macro economy has increased in the Region, it has not been reflected in the Health Care sector. Lack of resources due to insufficient funding results in poor exposure to clinical material on the wards and poor and inadequate facilities in theatre which are not conducive to good surgery let alone good training. In some Teaching Hospitals lack of basic equipment such as instruments, dressings, theatre drapes, etc., compound the problem together with insufficient support staff, such as nurses and lab technicians. Lack of funding for resources, both human and material, is a major factor in holding back progress not only in surgery but across the whole of the health care sector. It is a sad fact that in at least one country within the Region there is, at any one time, 50% absenteeism amongst health care workers and this mainly involving nurses and clinical officers who are ‘moonlighting’ to earn more money.7 However, at the end of the day it is National Governments who have to budget adequately for health care. I appreciate that the confounding factor with regard to funding is that there are so many players in the field such as NGO’s, Mission Hospitals, the pharmaceutical industry, and links with institutions outside the country, that Governments are loathe to interfere with all this aid coming in and are just happy that these outsiders are partly doing their job for them. One day, all this aid will dry up and the chickens will come home to roost! Perhaps we do not make Governments in the Region accountable enough for their actions with regard to health care and maybe this is something that a Regional body such as COSECSA could publicise. Manpower capacity is a serious problem which has a marked effect upon training of both undergraduates and postgraduates. The severe shortage of doctors has prompted Universities to increase the number of medical students per year but without a commensurate increase in the number of trainers, this is counter-productive. Even with a moderately stable number of postgraduate trainees there is still a problem because of insufficient trainers at any one time, either because of sheer numbers or the fact that some are not committed to training and are thus not available. Shortage of manpower is a serious challenge. Private practice is important because it does keep consultants in the Region and without the ability to undertake private practice many would not be here at all! However, private practice should compliment not compete with Teaching Hospital commitments and in some instances this needs addressing. However, the shortage is not confined to doctors alone. There is also insufficient capacity amongst nurses especially in the operating theatres, and of radiographers, physiotherapists, laboratory staff, etc. The cause of the crisis in manpower capacity is, in the main, related to funding and is the reason why, for instance, many nurses seek employment outside the Region such as in the UK where they can command a least three times the salary for doing the same amount of work. Are postgraduates for service or training? The answer must be for both but the role of the trainee needs defining. Clearly there is overlap between education, training, and service but the service aspect must not completely obliterate education and training as almost happens in one or two Teaching Hospitals within the Region. In the UK, where there are problems with the time available for training due to the European Working Time Directive, there is an argument for at least partly separating training from service provision for limited periods of time. For example a trainee could spend three months in a day surgical unit or on the wards but without any other commitments. It may be that we do not have the capacity to do this in the Region but it is something to think about especially where some programmes are so service heavy. The lack of adequate remuneration, annual and study leave is reflected throughout the Region. In three countries I visited postgraduate students are paid by their Governments but in the other three a different story unfolds. In one they are not paid at all and rely on ‘moonlighting’ to pay their fees and living expenses. Some have joined the armed forces and others have some sponsorship from Mission Hospitals or NGOs. This lack of proper remuneration for working for the State is affecting recruitment. To say that postgraduate trainees are working for a University Degree and therefore do not need paying is totally disingenuous when they are providing a major service commitment on the wards and in theatres, especially for emergencies. We, as consultants, must be advocates for our trainees and act on their behalf. It cannot make sense for a post graduate to work, say, 8-10 hours in the Teaching Hospital and then in the evening ‘moonlight’ for four or five hours in order to earn money to pay their fees and board and lodging. This certainly would not be possible at all within the European Union. Whilst I appreciate that there is a different culture in Africa I still believe that it is a basic human right to be paid an appropriate sum of money for services rendered. I am prepared to be shouted down but I feel unhappy about the present situation. Three Teaching Hospitals have no formal annual leave at all. The Universities regard them purely as students and students do not get leave despite the fact that the majority are working flat out providing a service commitment. In three other Teaching Hospitals annual leave ranges from two to five weeks. This lack of annual leave is also against my principles. I feel that we have to adhere to acceptable working practices. I do not subscribe to the view that what happened 30 or 40 years ago should continue into the modern age. One factor that is very evident is that the current trainees are far more socially and family conscious than previous generations. Times change and the Profession must change with them. Study leave did not exist apart from in two Teaching Hospitals; one of which allowed two weeks during the whole postgraduate course and the other two weeks prior to exams. It would not create too much of a problem for all trainees to receive a defined number of days study leave per year. This must be agreed with the Educational Supervisor and furthermore what they actually do during their study leave must be planned, agreed, and vouched for at the end of the period. Trainee representation within Departments of Surgery was essentially non-existent apart from in one Teaching Hospital where a post graduate forum discussed issues and the elected Chairman spoke to the relevant department with some success. In another Teaching Hospital there was no representation but each post graduate student had a Consultant mentor with whom they had regular contact. As with trainee assessment the process of representation involves feedback which is the life blood of progress and should be encouraged and not spurned. Representation should be based upon the numbers of post graduate students per year and certainly each year should have at least one Representative on a Committee with a committed member of staff as Chairman who need not necessarily be the Head of Department. It is invariably the case that there will be at least one or two younger members of the Consultant staff who will have a genuine interest in trainee welfare and would be keen to act as Chairman. Regular meetings should take place and matters can be referred to the Head of Department if and when needs be. Representation should not be seen as a threat. Furthermore, I believe that it would be in the interest of COSECSA to have at least one or two trainee representatives on Council. This may at first sight seem out of this world but I can assure you that in the UK the Royal Colleges and the Speciality Associations have for some time had trainee representatives on their Councils and their views are welcomed on issues that affect trainees, such as the Working Time Directive, training programmes, examinations, study leave entitlement, working practices, etc. Again, COSECSA should not feel threatened by this move. This is progress and should be welcomed. The MMed is mandatory in that it is the definitive programme with regard to obtaining a consultant appointment. There is a conflict of interest between the MMed and MCS programmes and this is difficult to resolve because essentially they are two competing systems. However, the MMed is not uniform from one country to another. In some Universities one can only train in general surgery whereas in others neurosurgery, urology or orthopaedics are an option. In some Universities the course is four years and in others five. However, at the end of training the postgraduates obtain a Degree. The MCS takes two years and results in a Diploma. Some Teaching Hospitals do not see the point in encouraging post graduate students to sit the MCS in addition to an MMed. Furthermore, if one has an MMed alone then one can sit the FCS without having an MCS. Some countries have essentially ignored the MCS and others have taken it up with enthusiasm. I suspect that COSECSA needs to see how the MCS beds down over the next three to five years because it is still early days. The MCS is important because it is a Regional exam whereas the MMed is a local “in country” exam. As I have already intimated there are wide variations between countries with regard to their MMed examinations whereas there is uniformity with regard to the MCS. However, at the present time 100% of the trainees I interviewed will be taking their MMed or the equivalent whereas only 20% will have taken or intend to take the MCS. The situation with regard to the FCS is quite different. There is no competing Diploma or Degree and the majority of trainees feel that the FCS in the various specialities works well. Sixty four percent of interviewees intend to or have taken the FCS. find the latter encouraging. At the end of the day it is hoped that all higher specialist education and training will take place within Region. At present this is not possible for all specialities and some post graduate students have to seek appropriate training abroad. THE FUTURE FOR COSECSA “The Mission of the College of Surgeons is to promote excellence in Surgical Care, Training and Research” My only slight quibble with this Statement is that it is difficult to quantify ‘excellence’ and I might suggest that we add the words ‘standards of’ in front of ‘excellence’ because it is possible to measure standards in a meaningful way. COSECSA has come a long way since its inception nine years ago and we must build upon undoubted success. One of the advantages of COSECSA is that it is a Regional College and thus is not influenced by any one particular constituent country. I believe we must drive through changes with regard to education, training and standards. We must use recognition of posts as a lever to improve training and make it more uniform across the Region. Regional services and specialisation go hand in hand. There has to be dialogue with the constituent countries and specialities with regard to what the perceived needs are at any one time. It may be that in one country there is a need to develop paediatric surgery and to do so might require, say, two extra Consultant Paediatric Surgeons and this therefore needs planning and executing accordingly. COSECSA needs to act as a hub for specialist training by recognising and supporting Centres of Excellence. If there are no immediate Centres for certain specialities then COSECSA should identify those outside the Region which would be suitable for appropriate training but the aim would eventually be for every speciality to have one or more Centres of Excellence within the Region. I believe that COSECSA should be the Regional Co-ordinator for incoming trainees from outside the Region who would have the added bonus of increasing capacity. Because of the perceived difficulty of training in the UK there are an increasing number of UK trainees who would value coming to the Region to gain practical experience. I emphasise that these would not be competing with trainees within the Region and hopefully in the future it may be possible to arrange an exchange whereby a UK trainee could swap with a trainee here. The UK are currently upgrading the Medical Training Initiative for overseas trainees who will be able to spend a maximum of two years in the UK with appropriate registration and full NHS pay. COSECSA needs to be the Regional centre for recruiting postgraduate courses, lecturers, bursaries, grants, etc. For instance the WHO recently had three bursaries to award to our Region within the field of burns and rehabilitation and there was some question as to where these should be allocated. Surely COSECSA should decide because they know the Regional scene intimately. COSECSA should also act as a consortium for surgical research. I have already mentioned the enormous potential for research in the Region and I appreciate this is going to take skill to achieve but the demand is there. If one reads a Medical Journal from the Region you will see that maybe nine out of ten papers will have been sponsored by an outside source such as a Research Institution or an NGO. In a Surgical Journal I doubt if you would find one publication supported by an outside source. We do ourselves a great disservice by ignoring the potential for research and this is an area that COSECSA must pursue. COSECSA needs to have a view with regard to Clinical Officers practicing surgery. The majority of countries in the Region either utilises or have utilised Clinical Officers as surgical practitioners at one time or another and this for good reason. In Tanzania, with a population of 36 million, there are 100 trained surgeons with roughly one third practicing in the cities, one third having an administrative position, and one third having emigrated, leaving one surgeon for approximately one million population11. In Ethiopia the ratio is approximately one surgeon to half a million population assuming that all surgeons are actively practicing in the country which is probably not the case. 12 The argument for training Clinical Officers in emergency surgery in some countries is indisputable13 . With adequate training and supervision they have been shown to perform as well as qualified surgeons, albeit in rather defined areas of practice, as was shown in Mozambique14 and Tanzania15 . However, it is true to say that some Clinical Officers feel more comfortable doing, say, a Caesarean Section which employs a standard technique than a laparotomy for peritonitis where they do not know what they are going to find. However, emergency Caesarean Sections are not necessarily easy operations and without adequate experience huge damage can result such as the development of a vesicovaginal or rectovaginal fistula. Nevetheless, Clinical Officers are cheaper to train than surgeons and remain not just in country but up country which is where emergency surgical expertise is needed. Some Training Hospitals also use Clinical Officers to man emergency surgical rotas. However, it is not just a matter of training them on a one off basis for there must be regulation, adequate support, supervision, on-going training and commensurate remuneration. My reason for saying that COSECSA needs to have a view with regard to Clinical Officers practicing surgery is that if countries are going to adopt this path in a significant way then COSECSA needs to be involved in their training which would further add to our manpower problems with regard to trainers. However, I would not wish to support the view that a high maternal mortality is due purely to a lack of surgical expertise. If a woman develops obstructed labour 150 miles from the nearest hospital and there are no roads and no transport and the only means of getting there is by walking, then it does not really matter whether there are one, ten or one hundred surgeons in the hospital 150 miles away for the woman will succumb on the journey. In other words, infrastructure goes hand in hand with appropriate surgical expertise. COSECSA is uniquely placed to disseminate best practice. Throughout the world there is a tremendous tendency to keep trying to reinvent the wheel. If one country has developed a technique for coping with a lack of resources which has proved successful then that needs to be disseminated throughout the Region so that all may learn and benefit. Audit is a very useful tool for improvement. COSECSA should maintain dialogue with outside organisations such as sister Colleges of Surgery, the WHO, the Tropical Health and Education Trust (THET) in the UK, Speciality Associations such as the ASGBI, Industry such as Ethicon, Research Institutions and with sympathetic Governments overseas. Networking achieves nothing but positive results. However, for COSECSA to succeed in the ways that I have outlined it is going to require the resources to do so. One suggestion is to invite Corporate Patrons to support the College. There are a number of prestigious institutions within the Region such as banks, cellphone distributors, IT producers, the pharmaceutical industry, and many others who need to be approached for their support and in exchange would receive free publicity. A website is important and the current one needs expanding but maintenance is expensive. However, this may be an area which a Corporate Patron could take under its wing. COSECSA can raise money by subscriptions alone or by also having a non-charitable wing which could produce diaries, calendars, insurance and travel facilities, etc., all involving publicity. These thoughts have not just come out of my head for they are the sort of areas that we in the UK have explored and have proved very successful. SUMMARY This lecture has been on education and training within the COSECSA Region and I have covered the background to the subject, the current situation, reported on certain problem areas, proffered possible solutions and finally have discussed the future. I conclude by stating that COSECSA has many friends and a number are actually here in the audience today – John Orr (President of the Royal College of Surgeons Edinburgh), Frank Keane (President of the Royal College of Surgeons in Ireland), Jimi Coker (Chairman, Overseas Surgical Fellowship Committee for the Association of Surgeons of Great Britain and Ireland), Denis Robson (Director of African Affairs) and Steve Brockie (Sub Saharan Africa Business Manager), both of Ethicon (a Johnson & Johnson Company), George Borthwick and Lindsay Stewart, previous Managing Directors of the same Company and Andrew Howard, Director, Office of International Surgery, University of Toronto. I have enjoyed enormously the opportunity to visit trainees across the Region and have been impressed by their commitment and resilience, sometimes against all the odds, such as in Zimbabwe, that it has been a humbling experience. I am confident that surgery in the Region will develop in the way that we should all wish and this through the continued efforts with regard to education and training by our College of Surgeons of East, Central and Southern Africa. Thank you. REFERENCES
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09001f3.jpg] [js09001f2.jpg] [js09001f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}