 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
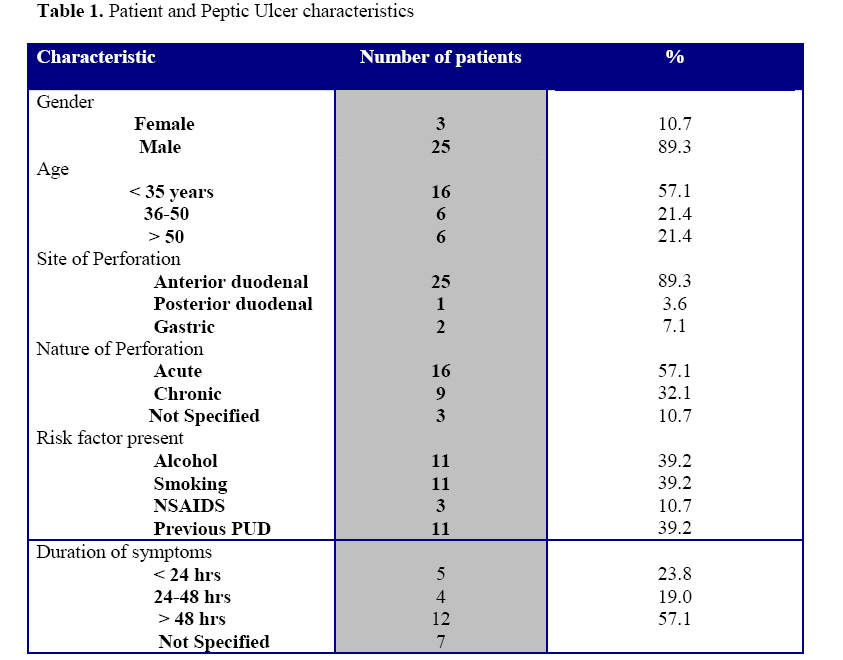
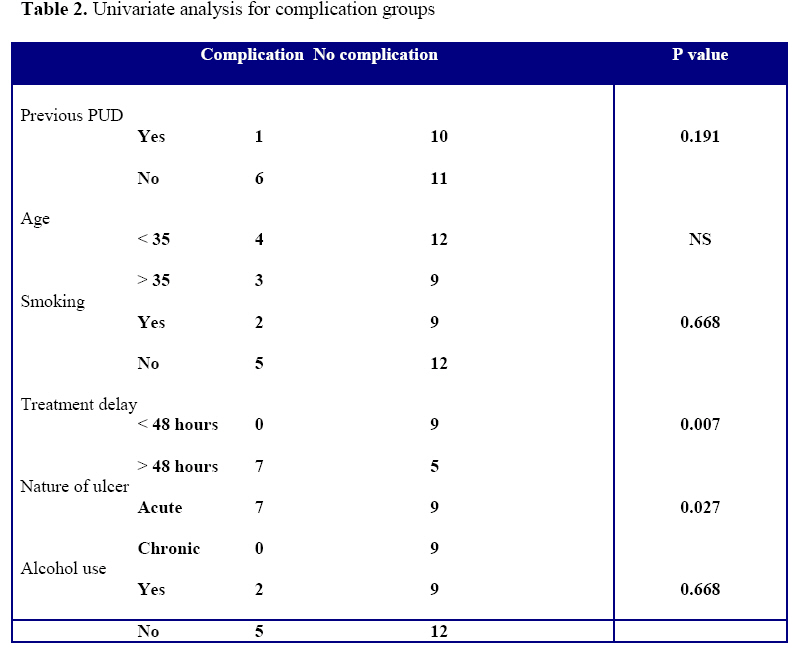
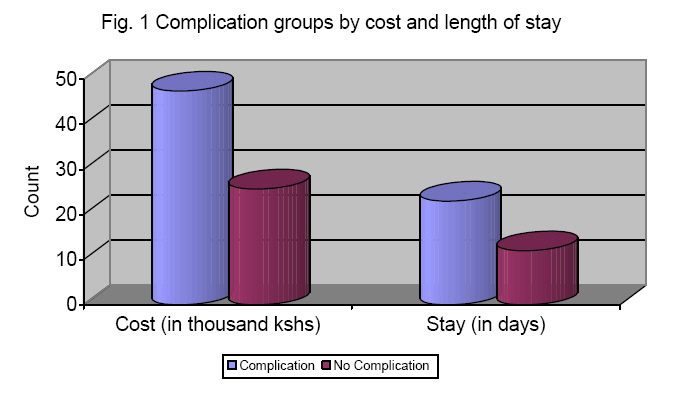
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 13-17 Perforated Peptic Ulcer Disease at Kenyatta National Hospital, Nairobi. N.A. Nasio1, H. Saidi1,2 1Department of Surgery, 2Department of Human Anatomy, University of Nairobi Code Number: js09002 Background: Published reports on perforated peptic ulcers indicate increasing rates for the elderly, those chronically ill and females. Our local observations are at variance. This study analysed patients treated for peptic ulcer perforations at the Kenyatta National Hospital between January 2005 and December 2006. Introduction The introduction of antisecretory drugs in 1970 and later, proton pump inhibitors have, in addition to eradication of Helicobacter Pylori infection, changed both the treatment and outcome of peptic ulcer disease1,2,3,4. Although the rate of elective peptic ulcer surgery has dramatically reduced as a result, emergency operations for perforations have remained constant or increased2,5. The mainstay of treatment in perforations has remained the omental patch repair with peritoneal lavage6,7 although laparoscopic repairs are being popularized in some institutions8,9,10,11,12 . Published reports on perforated peptic ulcer disease, especially from Western countries, indicate higher rates of perforations for the elderly, those chronically ill and an increasing female involvement5. Our local observations do not seem to support this trend in admissions. The aim of this study was to describe the pattern of perforated peptic ulcers (PPU) at the Kenyatta National Hospital in Nairobi over a 2-year period. Patients and Methods This was a retrospective review of patients operated for peptic ulcer perforations Kenyatta National Hospital (KNH) in Nairobi from January 2005 to December 2005. KNH is the main national referral hospital. The 2,000 bed hospital is also the teaching facility for the University Of Nairobi School Of Medicine. Clinical charts of 44 patients operated for perforated peptic ulcer from January 2005 to December 2006 were reviewed. Sixteen cases were excluded from this study because of incomplete patient and clinical data in their charts. The surgical procedure for all the patients involved refreshing the perforation, repair with interrupted sutures, placement of a Graham patch and peritoneal lavage. Data extracted included demographic data, clinical presentation, and time from symptom onset to treatment, risk factors and in-hospital complications. The information was entered in pre-coded data sheets and summarized in the form of proportions and averages. The complication groups (present or absent) were compared for the prevalence of risk factors, gender groups, treatment delays and age. The X2 analysis and the Fisher’s exact tests were used for categorical and continuous data as appropriate. Results Out of the 44, 28 patients (retrieval rate of 63.6%) had complete data and were analyzed. The male to female sex ratio was 8.3:1. The patients’ ages ranged from 11 to 78 with a median of 35.4 years. The majority (57.1%) of patients were aged 35 years and younger (Table 1). The patients’ occupations included semiskilled casual laborers, students, informal businesses and the unemployed. The most common presenting complaints were sudden onset abdominal pain and vomiting. The duration of symptoms ranged from 1 to 14 days, the mean duration was 7.5 days. Three patients (10.7%) gave a history of regular ingestion of non-steroidal anti-inflammatory drugs for joint and back pains. Other risk factors recorded included alcohol consumption in 11 patients and smoking in 11 patients as well. Most patients who smoked also took alcohol. A similar proportion of patients (39.3%) reported previous treatment for peptic ulcer disease. Patients with a previous history of PUD (peptic ulcer disease) had had symptoms for durations ranging from 2 to 28 years. The treatment pattern was predominantly the use of variety of antacid mixtures for symptomatic relief. One patient was presenting with a re-perforation. Most of the perforations were anterior and duodenal (Table 1). Histology of the biopsy specimens revealed no malignancy. There were 9 reported chronic ulcers and 16 acute ulcerations. All biopsies were not stained for Helicobacter Pylori There were 4 deaths out of 28 cases, giving a 14.3% mortality rate. Complications were recorded in 7 patients (25%). These complications included 3 cases of wound sepsis, 3 reperforations/leaks and 1 re-operation for burst abdomen. Five patients had blood transfusion ranging from two units to six units of whole blood. Four of the 5 patients who received blood transfusion died. The factors which were significantly associated with complications were treatment delay (p=0.007) and acute perforation (p = 0.027) (Table 2).The age, previous history of PUD and other associated risk factors did not significantly influence the rate of complications. The duration of hospital stay ranged from 3 days to 79 days with an average of 15 days. The associated treatment cost was Kshs 29,701.409 (range 5,580-77,150 Kshs). The treatment cost was higher for the group of patients who developed complications. (Figure 1). Patient follow–up was poor. Only 5 patients (17.8%) revisited the surgical outpatient clinic for post-operative evaluations. Discussion The observations of the current study indicate a predominant male association for perforated peptic ulcer disease. The patients presented late with attendant significant morbidity and mortality. The delay was also associated with increased cost of treatment and lengths of stay. The mortality rate of 14.3% in this study is higher than the 2.7 to 13.8% rates reported by Boey et al13 . This high rate may be attributed to the long time interval between perforation and initiation of treatment. The majority (57%) of patients in our study had treatment 48 hours after the onset of symptoms. The reasons for the treatment delays were not clear. This could have both pre-hospital and intra-hospital components. Patient choices are an important cause of treatment delays. Hospital treatment is expensive and the patients may seek care only when the pain is unbearable. Patients may take medications in the pre-hospital period with hope that the symptom will abate. It is also possible that some clinicians managing the patients initially may not have considered perforation as a possible diagnosis. The specific patterns and reasons for delay need to be investigated. The predominance of young males in the present study is similar to other studies from the developing world. For instance, Tessema et al14 in Ethiopia found a mean age of 32.6 years and a male to female sex ratio of 7.2:1. As expected, most of the perforated ulcers were in the anterior duodenum. The duodenum within 1-2 cm of the pylorus is the first portion of the intestine first exposed to gastric secretions. Only 3.6% of perforations were identified as posterior duodenal. Studies indicate that the latter site is associated with brisk haemorrhage from the gastroduodenal artery that may manifest with volume depletion and higher complication and mortality15 . The choice of operative procedure in the current series was limited to omental Graham patch repair. Although this procedure has been associated with ulcer recurrence rates of up to 40%, the significant side effects of definitive ulcer surgery (dumping in 50% and diarrhea in 10%)16 and the advent of efficacious medical treatment (proton pump inhibitors, H2 receptor blockers H. pylori eradication), and triple therapy, the patch repair will remain popular. Incidence of H. pylori peaks 80-92% in patients with perforation17 and its eradication is pivotal. In one randomized study, patients put on PPI alone were compared to those whose therapy included H. pylori eradication. The recurrence rates were 38.1% and 4.8%, one year after simple closure of duodenal perforation17. For the group of patients in the current study, definitive acid-reducing procedures (gastric resection or vagotomy and pyloroplasty) were not an option because of the late-presentation. These procedures are contraindicated in patients who are hemodynamically unstable, have diffuse peritonitis or have multiple co-morbid conditions15. No patient underwent laparoscopic repair. Established in the 1990s, studies have confirmed its efficacy for small perforations18. It offers advantages in terms of reduced analgesic requirements, faster return to oral feeding, faster return to normal daily activities and reduced morbidity and chest complications. Conclusion Perforated peptic ulcers are a disease of young males, risk factors were documented for significant proportion of patients. Efforts to reduce delay in presentation in this population may reduce the complications. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09002f1.jpg] [js09002t1.jpg] [js09002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}