 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
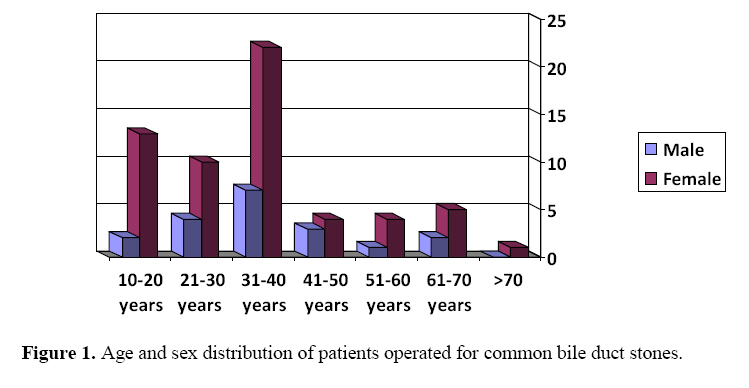
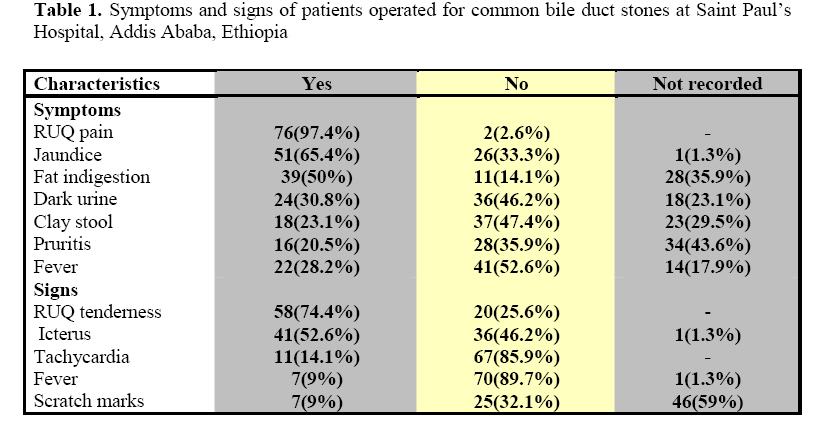
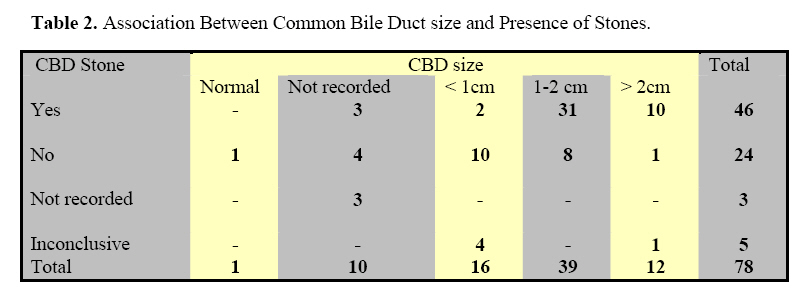
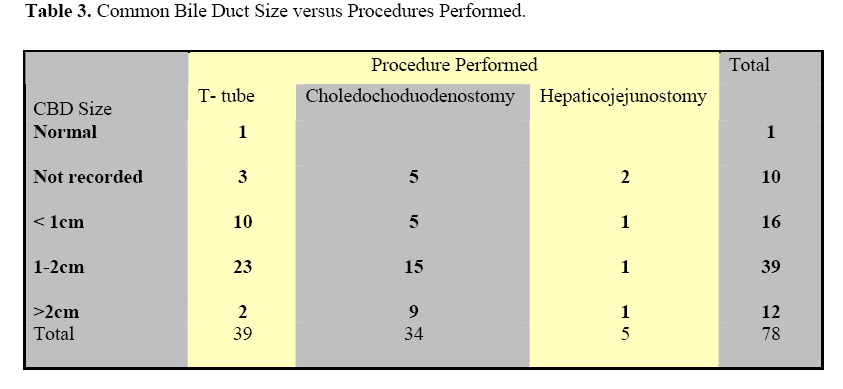
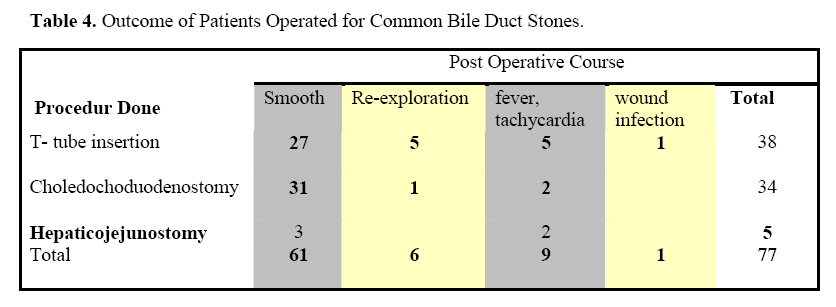
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 18-23 Surgical Management of Common Bile Duct Stones at Saint Paul’s Hospital, Addis Ababa, Ethiopia S. Kassa, B. Kotisso, A. Deneke. Addis Ababa University, Faculty of Medicine, Department of Surgery. Code Number: js09003 Background: This study was aimed at evaluating the trend and outcome of surgical management of choledocholithiasis in St. Paul Teaching Hospital Addis Ababa, Ethiopia. Introduction Common bile duct (CBD) stones are detected in 8% to 16% of patients who have cholelithiasis1. About 500,000 gallbladders are removed in the United States annually. The CBD is explored in nearly one quarter of them, and stones are removed in about two-third of these explorations 2. A report from Japan indicates that incidence of choledocholithiasis is even higher occurring in 18.5% of patients operated for cholelithiasis3. Biliary lithiasis is not uncommon in the developing world too. A report on pattern on admission to the surgical department of Tikur Anbessa hospital (TAH)4 revealed that cholelithiasis and its complications accounted for 10% of the whole admission and 25.9% of GI conditions. Bekele5 reported overall 12.35% of CBD exploration in 712 cholecystectomies in Ras Desta hospital, Addis Ababa. On another study from the same hospital, Choledocholithiasis accounted for 41% 0f obstructive jaundice cases6. A study from Tikur Anbessa hospital revealed that CBD stone was found in 8% of 745 patients who underwent Cholecystectomy for cholelithiasis7. The traditional open surgical management of CBD stone is choledochotomy and stone removal with T-tube placement, which may be kept for a minimum of 10 days before removal provided that complete evacuation of the stone is ascertained1. Sides to side choledochoduodenostomy and choledochoduodenostomy transduodenal sphincteroplasty are other options with their own indication and contraindications8 . Since 1891, when Sprengel did the first side to side choledochoduodenostomy, choledochoduodenostomy (CD) has had varying degrees of popularity because of possible complications such as recurrent abdominal pain or cholangitis which has been termed as the “sump syndrome”9,10. However, the recent trend is that surgeons in America, Europe and else where have shown interest in the procedure after analyzing its favorable long term outcome and clearly the indications for constructing3,10,11,12,13. There are no studies done in Ethiopia in line with the practice of CD. This retrospective study is undertaken to assess the pattern and outcome of surgical management of choledocholithiasis and compare the pitfalls of the different procedures used in one of the tertiary level hospitals in the capital city, Addis Ababa, Ethiopia. Material and Methods Saint Paul’s hospital is a tertiary level hospital in Addis Ababa, Ethiopia, with 130 surgical beds. The study is a clinical based retrospective analysis covering a period of five years from January 1st 1994 to December 30 1999. The operation registry book was used to identify the cases that were operated for biliary lithiasis. Then the records where obtained from the record office of the hospital and data were collected in a predesigned format. A total of 1230 patients underwent Cholecystectomy during the study period among which 98(7%) had choledocholithiasis. Of the 98 patients with choledocholithiasis the records of 78 (79%) patients could be retrieved and made the basis for this study. Included variables were, Socio-demographic data, preoperative diagnosis, intraoperative findings and the type of procedure, postoperative hospital stay, complications and follow-up course. Data was analyzed by SPSS statistical software. Pearson’s chi-square test was used for statistical analysis. P value <0.05 was considered significant. Results During the study period, 1230 patients underwent surgery for cholelithiasis among which 98(7%) had choledocholithiasis. The records of 78 (79%) patients was retrieved and made the basis for this study. Fifty-nine (75.6%) patients were females and 19(24.4%) were males, with a female to male ratio of 3.1:1.The mean age was 49 years with range of 16 to 87(Figure 1). As is shown in Table 1 the most common presenting symptoms were right upper quadrant pain, jaundice, fat indigestion in 76 (97.4%), 51(65.4%), 39(50%) of the cases respectively. Right upper quadrant tenderness and icterus were the most frequent physical signs observed in 58(74.4%) and 41(52.6%) respectively. The laboratory serum bilirubin and transaminase levels along with ultrasound of the abdomen were the diagnostic aid used apart from history and physical findings. The admission diagnosis of choledocholithiasis with or without jaundice was made in 59 (75%) of the patients. Ultrasound of the biliary tree was the diagnostic facility used to evaluate the CBD. The size of the CBD was recorded in 68 cases and was above 10mm in 62(91%)of the cases. CBD stone was clearly picked on ultrasound in45/78 (57.7%) (Table 2). The type of the procedure and CBD size is indicated in Table 3. Choledochotomy with T-tube drainage and choledochoduodenostomy were the two frequently performed procedures. Although it seems that bigger duct size might have pressed to do choledochoduodenostomy the distribution is not significantly different. The type of the procedure and CBD size is indicated in Table 3. Choledochotomy with T-tube drainage and choledochoduodenostomy were the two frequently performed procedures. Although it seems that bigger duct size might have pressed to do choledochoduodenostomy the distribution is not significantly different. The postoperative stay was significantly delayed (p<0.019) for the choledochotomy and T-tube drainage group. .Re-exploration rate was also more in the T-tube drainage group. On follow up three of the T-tube drainage and one of the choledochoduodenostomy patients got complicated which deserved re-exploration which is not statistically significant. (Table 4). Discussion Choledocholithiasis comprised 7% of all cholelithiasis cases which compares well with the 816% that is reported in the literature1,,2,5-7 . The CBD stones are, in most instances secondary to gallstone. Primary choledocholithiasis are found under some circumstances. The high female preponderance observed in our study is a known fact and is in relation with other studies1-3, 5,6,7,8 10-12. Our patients with a mean age of 49 years were younger that found in most studies8,10-12 but was similar to what Bekele5,6 and Tessema7 reported. Our finding of right upper quadrant pain and Jaundice as leading symptoms is in line with other studies5,6,7 . Similarly Icterus and right upper quadrant tenderness were the frequently identified signs, which is in agreement with observations by other investigators6,10 . Ultrasonography is said to be unreliable in the detection of stone in the common bile duct1. In our case it could peak 58 % of the choledochal stone, which goes with the conclusion reached earlier1. There still remain controversies, how best to handle choledocholithiasis. The classical CBD exploration and T-tube drainage is accompanied by various complications including incomplete evacuation, bile leak and sepsis and recurrent stone3. On the other hand recurrent choledocholithiasis remains a challenge for both the patient and the surgeon. Recurrence rates as high as 10% have been reported after a second operation on the biliary tract. Sterling had reported that re-exploration of the CBD is associated with a mortality that is twice that for the initial choledochotomy and four times that for an uncomplicated cholecystectomy14 . These facts compelled the surgeons, in different countries; to look for an operative procedure option with minimal postoperative complication and better long term out come with no or little recurrence rate. It was mandatory to revisit side-to-side choledochoduodenostomy, which was abandoned for the fear of sump syndrome9. However long term follow up of patients with this procedure could not substantiate the fear3,11,14-17 . On the contrary, almost all the studies showed that the immediate postoperative complications were significantly less in the choledochoduodenostomy group as compared to Ttube drainage. The need for re-exploration for recurrent lithiasis was high for the T-tube group. In a recent report by Zhe-Fu Li and Xio-Ping Chen from China, recurrence rate was 8.6%after T-tube drainage while it was only 2.45 after CD (p value < 0.05)18 . Our observation is in line with these authors. Postoperative stay was significantly delayed in those with T-tube drainage (P value < 0.019). Re-exploration in the early postoperative period was also more for the T-tube drainage group though not statistically significant. On long term follow up, too, more complication was noticed for T-tube drainage. This observation definitely favors Choledochoduodenostomy for surgical management of properly selected cases of common bile duct stones. The indications to do CD include Size of CBD, ampullary stenosis, multiple calculi, retained or residual stone, hepatic stones, distal CBD stricture, recurrent common duct stone, impacted ampullary stone, primary common duct stones etc8. Most authorities in the field recommend a CBD size of 15mm and above10-17. Some believe that CD can safely be done with CBD size as small as 10 mm. In our case we noticed that CD was performed even in CBD sizes less than 10 mm. Most of our patients had smooth postoperative course and had no significant complication on further follow-up. One may be tempted to conclude that CBD size might matter little. However, as it is technically demanding and inconvenient we don’t recommend doing CD where the size is less than 10 mm. It would rather be advisable to stick to a size of 15mm and above. Conclusion In conclusion this study has shown that side-to-side CD is a better alternative procedure with less early and late complication. We recommend it for multiple CBD calculi, much dilated CBD (2cm), big stone in the CBD, Hepatic stone, recurrent stone, Primary CBD stone and elderly patients where the size of CBD is 15mm and above. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09003t2.jpg] [js09003t4.jpg] [js09003t1.jpg] [js09003t3.jpg] [js09003f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}