 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 24-31 Are Clinicopathological Factors Predictive of Bactibilia in Biliary Tract Diseases? A.B. Khan1, S.A. Salati 1, A.B. Khan 2, B.K.Parihar3 1Assistant Consultant, Dept of Surgical Specialities, King Fahad Medical City, Riyadh` KSA. Code Number: js09004 Background: Biliary tract disease is very common in Indian side of Jammu and Kashmir and because of this we got prompted to undertake a study to find out the association between presenting features and bactibilia. Introduction Aspiration and culture of bile at the time of biliary surgery provides a unique opportunity to study biliary bacterial flora as this may have diagnostic ,prognostic or therapeutic implications1.Under normal conditions bile, biliary tree and liver are sterile2,3 but it becomes colonised in biliary tract disease. The precise origin of biliary bacteria is not known. The possible explanations being ascending infection from duodenum, lymphatic spread and vascular spread from portal venous or hepatic arterial flow or seeding from chronically inflamed gall bladder4.The micro organisms most often implicated in infected bile include Escheriachia coli, Klebsiella and Entrococcus species along with gram positive cocci and anaerobes like anaerobic streptococci ,Bacteriodes fragilis and Clostridium welchii5,6.The reported incidence of bacteria in bile is highly variable ranging from 8% -42%7,8,9.The reasons for these enormous variations include type of patients being studied and use of antibiotics preoperatively. The single dose of preoperative antibiotics does not render the bile sterilize10.Host of previous studies suggest that biliary surgery is attended by high risk of septic complications11,12.The aim of our study was to identify the bacteria present in bile in biliary surgery and try to find the risk factors predictive of bactibilia. Material and Methods This prospective study was conducted in the Department of Surgery, Government Medical College Jammu, India over a period of one year from March 2003-February 2004 and included 121 patients undergoing various biliary procedures who gave an informed consent. Patients in study included those with:
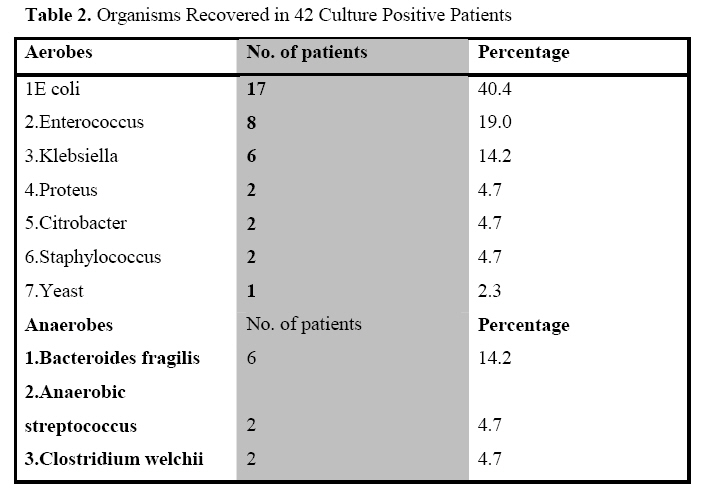
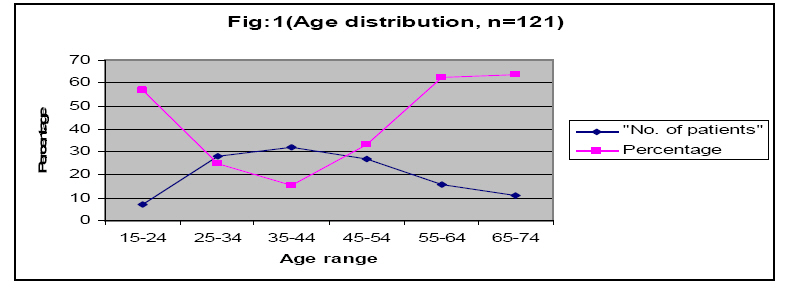
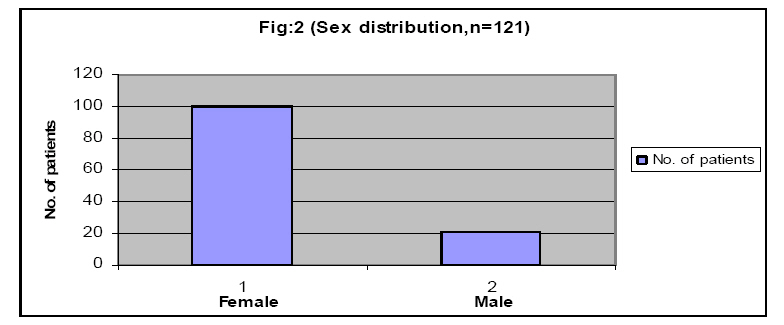
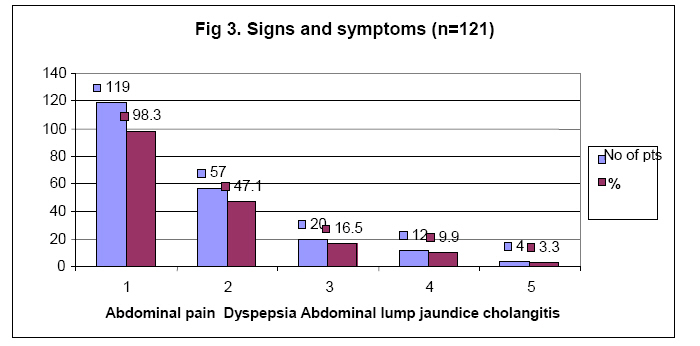
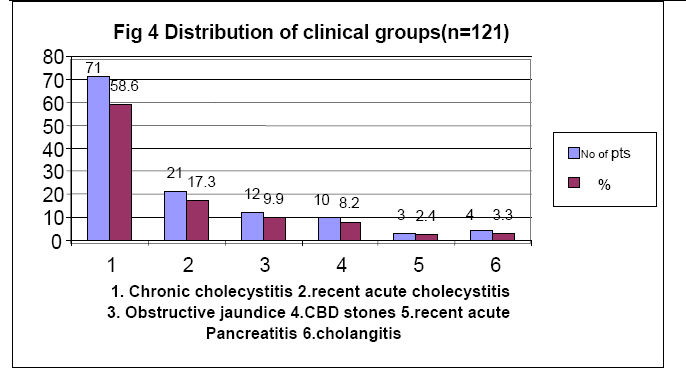
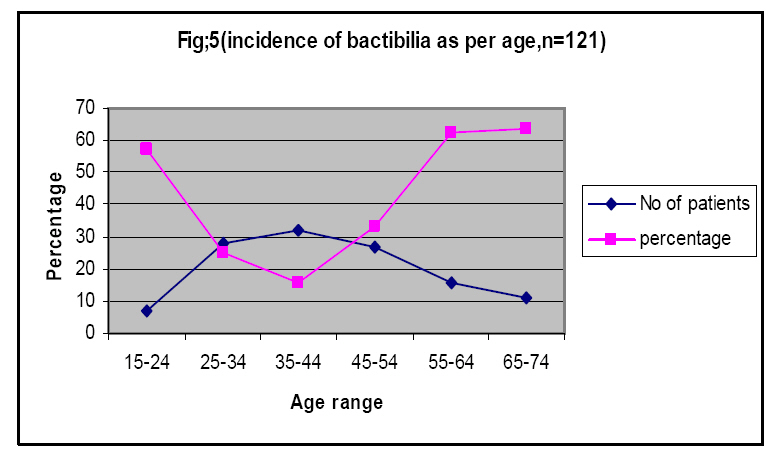
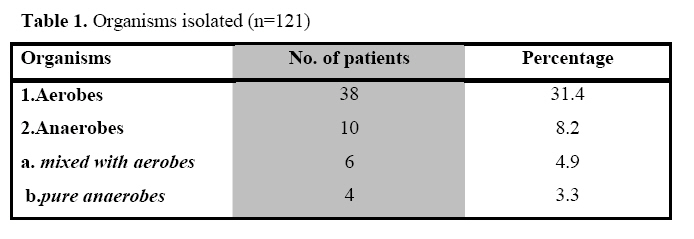
In open cholecystectomy the bile was aspirated into a syringe after removal of the viscus while in laparoscopic procedures it was bile aspirated percutaneously by spinal needle after scope was introduced. Bile from common bile duct was obtained by direct puncture. About 3-5ml of bile was drawn with needle, immediately capped and samples transported immediately to microbiology laboratory for analysis. Direct smears of the samples were stained by gram staining (Hi media) and examined under microscope. For aerobic cultures, samples were inoculated on Sheep blood agar and MacConkeys agar medium and incubated at 37 degree centigrade overnight. For anaerobic cultures, samples were inoculated on neomycin containing blood agar medium. A disc containing metronidazole was placed over primary inoculation and the plate was then placed in gaspak jar (Hi media) and incubated at 37 degree centigrade for 48 hours. The growth on the media was identified by colony characteristics and standard biochemical identification scheme (Stokes).Post operative cultures in patients with T tubes were repeated on 4th-7th day. All the patients included in this study were given single dose of preoperative antibiotic at the induction of anaesthesia and antibiotics changed postoperatively depending on the culture and sensitivity report. Results The age range of our series of 121 patients was 15-74 years with a mean age of 42.5 years. There were 100 females and 21 males with male to female ratio of 4.7:1. Our patients presented with varied symptoms and signs with abdominal pain the commonest symptom(98.3%) followed by dyspepsia(47.1%), abdominal lump(16.5%), jaundice(9.9%) and cholangitis(3.3%).Most of the patients had more than one presentation. Our series of 121 patients were distributed in following clinical groups with the largest clinical group being the chronic cholecystitis (58.6%), recent acute cholecystitis (17.3%),obstructive jaundice (9.9%),CBD stones without jaundice (8.2%), recent acute pancreatitis (2.4%) and cholangitis (3.3%). The most common operative diagnosis was cholelithiasis with chronic cholecystitis (58.6%) followed by choledocholithiasis(14.8%).Mucocoele was present in 11 cases (9%),resolving acute cholecystitis in 11 cases (9%),CBD stricture in 4 cases (3.3%) and empyema and gall bladder polyps accounted for 3 cases each, contributing 2.4% each. Gram staining of the bile smears for 121 patients showed organisms in 51 patients (42.1%) where as rest of the patients did not show any organism. Out of 121 cases 42 (34.7%) turned out to be culture positive and rest of the cases turned out to be culture negative. In culture positive cases aerobes were identified in 38 (34.1%) and anaerobes were identified in 10 (8.2%) patients. These organisms occurred in combination in various patients. The distribution of various organisms among culture positive patients is depicted below in the Table 2.
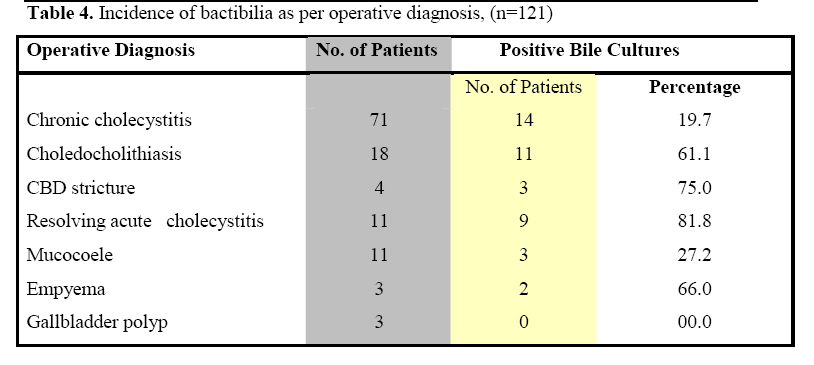
We examined the incidence of bactibilia as per operative diagnosis in these patients. Highest incidence of positive cultures was found in patients with operative diagnosis f resolving acute cholecystitis(81.8%) followed by bile duct stricture(75%).The distribution is shown in Table 4.
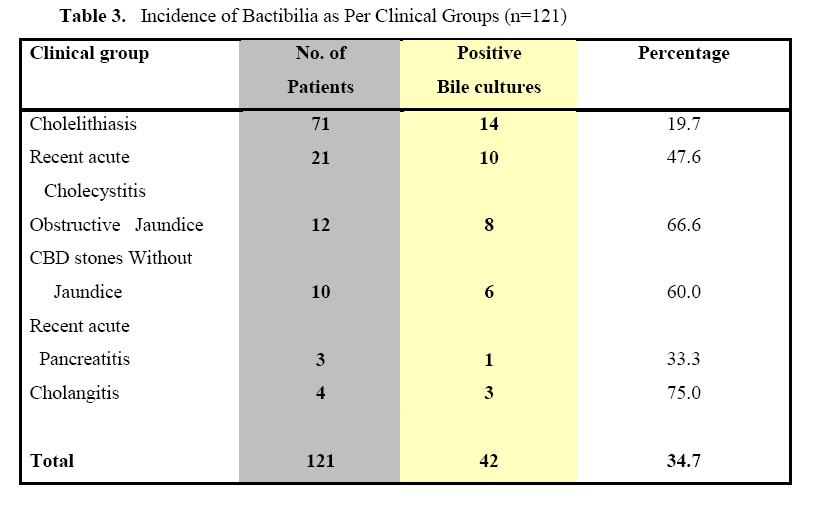
Discussion The main goal of this study was to assess the prevalence of micro organisms in bile in patients suffering from various biliary tract diseases so that a categorisation of the patients could be done as to who require prophylactic antibiotics. As evident from the results of the study the overall prevalence of positive bile cultures was 34.7% and the most common isolate grown from bile was Ecoli (40.4%) followed by Enerococcus faecalis (19.0%) and Klebsiella (14.2%).Anaerobic yield was 8.2% with the most common isolate being Bacteriodes fragilis. Our findings concur with the previous findings10,13,14,17 but number of other studies are at variance with the results of our study15,16 and this difference could be explained by different patient characteristic of study population The use of prophylactic antibiotic at the time of induction of anaesthesia in the present study did not sterilize the bile and did not reduce the incidence of bactibilia as the yield of micro organisms is similar to host of other studies18,19,20 . In present study gram staining correctly identified the presence and type of organisms in 72.5% of cases where as in 5% cases it was not able to identify organism correctly this is as per the previous study14 but at discord with another study21 which showed poor correlation between microscopy and culture. The result of the present study strengthen our belief that if significant number of bacteria are present in bile, they should be identified readily on uncentrifuged sample of bile where they may also be more easily distinguished from epithelial debris. We believe that the concept of using gram staining of bile should be similar to the concept of using frozen sections in breast disease. This has lent us to the belief that Intraoperative bile smears may be used as an early indicator to institute appropriate antibiotic therapy at the time of surgery22 . The results of the present study lend us to the view that preoperative characteristics of the patients are highly predictive of Intraoperative bactibilia. In present study the incidence of bactibilia was significantly higher in certain clinical groups which could be categorised as age>65, recent acute cholecystitis, common duct stones with and with out jaundice, recent acute pancreatitis and cholangitis.This is in accordance with number of previous studies10,16,23,24,25. So we consider it worthwhile to divide patients with one or more of these risk factors in high risk category and patients without these risk factors in low risk category. This has a clinical significance as in high risk group bile cultures are frequently positive where as in low risk group they are infrequently positive. Thus if high risk factors are identified preoperatively appropriate antibiotics could be instituted preoperatively. In accordance with previous studies8,15,26 we found that the operative findings provide a useful guide as to likelihood of bactibilia. In a previous study8 biliary sepsis was common in patients with jaundice and stones of common bile duct but unusual in stones confined to gall bladder undergoing elective cholescystectomy.In addition to this in the present study we got higher percentage of positive bile culture in resolving acute cholecystitis(81.8%), empyema(66,6%)and CBD stricture (75%). Conclusion In conclusion patients with biliary tract disease harbour bacteria in their bile. Patients could be stratified according to the presence of risk factors such as age>65, recent acute cholecystitis, recent acute pancreatitis, CBD stones with or with out jaundice, CBD stricture and cholangitis into high risk category and in absence of these risk factors in to low risk category. Low risk category patients should receive limited prophylactic antibiotics where as high risk patients should receive full therapeutic antibiotics to reduce the incidence of post operative sepsis. Intraoperative gram staining is an important tool to identify presence of bactibilia early before the results of culture are available and the culture should be done routinely and antibiotics modified according to the sensitivity report. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09004t4.jpg] [js09004t3.jpg] [js09004f3.jpg] [js09004f2.jpg] [js09004f5.jpg] [js09004t1.jpg] [js09004f1.jpg] [js09004f4.jpg] [js09004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}