 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
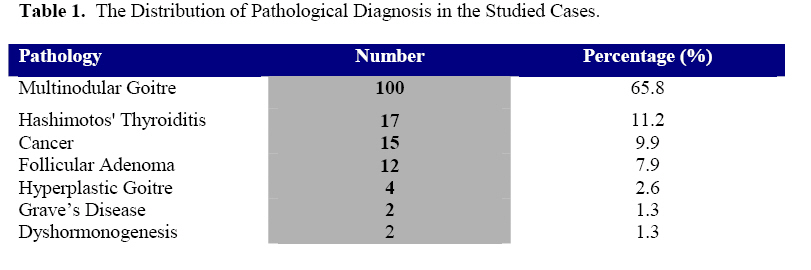
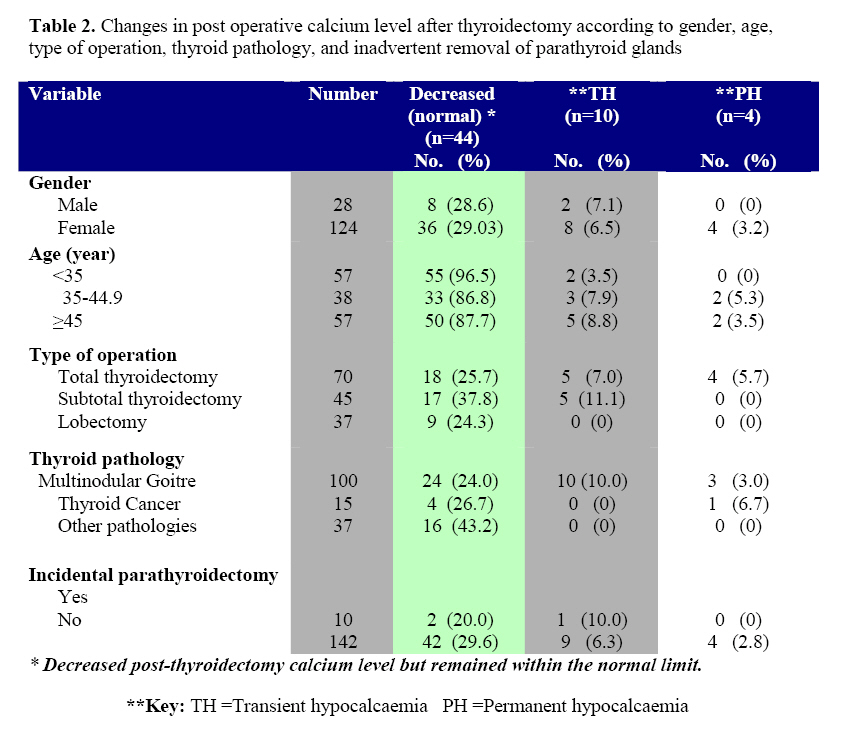
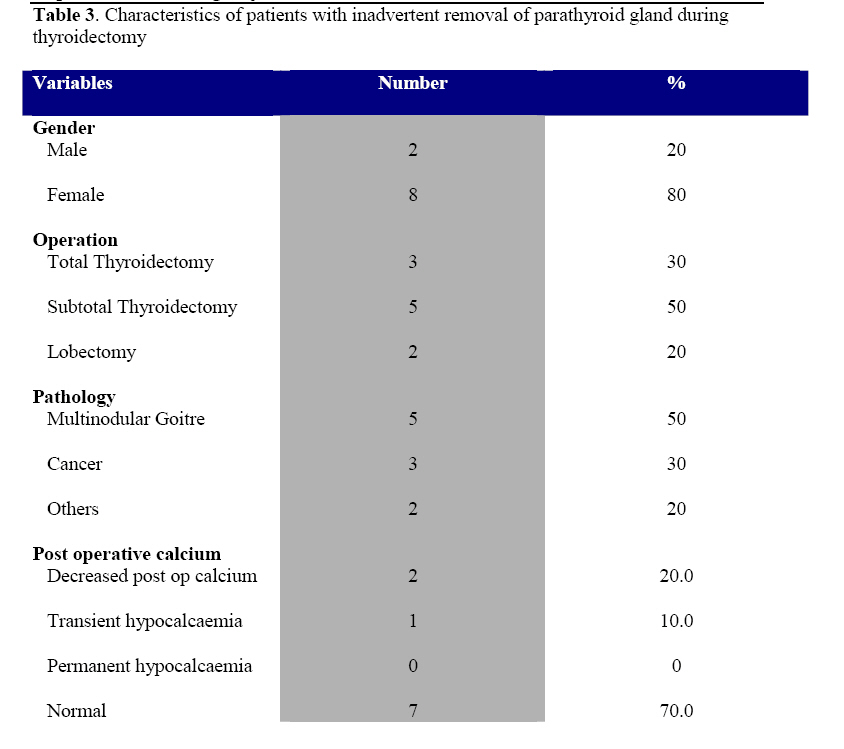
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 32-37 Post-thyroidectomy Hypocalcemia in King Abdullah University Hospital and Princess Basma Teaching Hospital, Jordan G.R. Qasaimeh1 , Y. Khader2 , F.M. Al-Mohamed3, A.K. Omari4 , A. Dalalah5 , 1Assistant Professor in General Surgery-King Abdullah University Hospital, Jordan University of Science and Technology. Code Number: js09005 Background: Thyroidectomy is one of the major and delicate operations commonly performed in surgical units. This study was aimed at determining the incidence of hypocalcaemia after thyroidectomy operation among patients who underwent thyroidectomy in two teaching hospitals in the north of Jordan. Introduction Thyroidectomy is one of the main operations performed in surgical units. The indications for this operation include cosmetic problems, obstructive symptoms, hyperthyroidism and clinical suspicion of malignancy1. The main postoperative complications of this operation are injury to the recurrent laryngeal nerve and hypocalcaemia2. The incidence of hypocalcaemia varies in different studies from 1.6% to 83%3. It usually manifests in the first 24 hours but some patients may not develop hypocalcaemia until four days post operatively4. In most cases it is transient hypocalcaemia (TH) that resolves spontaneously and only few patients develop permanent hypocalcaemia (PH)3. Prediction of patients at risk for the development of post-thyroidectomy hypocalcaemia enables the surgeon to closely monitor the patients at risk and permits earlier and safer discharge from the hospital of the patients who are more likely to remain normocalcemic5. Many factors have been implicated in the cause of post operative hypocalcaemia such as haemodilution, elevation of urinary calcium excretion, calcitonin release and hungry bone syndrome3,6 . The most probable cause in patients developing significant hypocalcaemia is hypoparathyroidism secondary to damage, devascularization, or inadvertent removal of parathyroid glands during thyroidectomy operation7. The aim of this study was to determine the incidence of hypocalcaemia after thyroidectomy operation among patients who underwent thyroidectomy in two teaching hospitals in the north of Jordan. Methods The medical records of 152 patients who underwent thyroid surgery in King Abdullah University Hospital and Princess Basma Teaching Hospital in the period between January 2003 and January 2007 were reviewed by the study team. The two hospitals are the main referral hospitals in north of Jordan and both are attached to the Medical College in Jordan University of Science and Technology. The study was approved by the review board in both hospitals. The patients included were those who underwent unilateral or bilateral thyroid operations. Patients with associated parathyroid pathology were excluded. The operations were performed by consultant surgeons and consisted of lobectomy, subtotal thyroidectomy or total thyroidectomy.The surgeons involved followed the same protocol adopted by the surgical department in the medical college regarding the surgical management of thyroid swellings. In all patients the recurrent laryngeal nerves and the four parathyroid glands were identified and preserved whenever possible. Ligation of the trunk of inferior thyroid artery was avoided and the blood supply to parathyroid glands was preserved as much as possible. In benign thyroid disease the resection was conducted intracapsularly to avoid damage to the parathyroid glands and their blood supply. In occasional cases when a parathyroid gland was accidentally excised during the operation autotransplantation in the homolateral sternocleidomastoid muscle was done. In the cases that underwent lobectomy, exploration of the opposite lobe was done routinely to exclude any occult pathology. The medical records were reviewed for age, gender, clinical diagnosis, extent of surgery, pathology reports, incidental parathyroid resection in pathology specimens, the preoperative serum calcium level, the post operative and the follow up serum calcium levels. Measurement of serum calcium level was done routinely pre-operatively, 24 hours and 48 hours postoperatively. It was repeated several times if the postoperative level decreased. Parathormone hormone level was measured postoperatively only in those patients who developed hypocalcemia. Hypocalcaemia was defined as serum calcium level less than 2.0 mmol/L on at least two consecutive measurements and in patients who became symptomatic for hypocalcaemia and required supplementation therapy of calcium and vitamin D. It was considered Transient (TH) if it resolved within six months and Permanent (PH) if it persisted after six months and the patient was maintained on supplementation therapy of calcium and vitamin D8. Data was recorded and analyzed using the Statistical Package for Social Sciences (SPSS, version 15). Data were described using frequencies and percentages. Results A total of 152 patients aged from 10 to 84 years with a mean (SD) age of 41.9 years underwent thyroidectomy in the period between January 2003 and January 2007 in two teaching hospitals in north of Jordan. Majority of patients (65.8%) had multinodular goiter (Table 1). They included 124 females and 28 males. The majority (65.8%) of the patients had multinodular goitre; 15 (9.7%) had thyroid cancer with 10 being carcinomas, 3 follicular carcinomas, one Medullary carcinoma and one lymphoma. Total thyroidectomy was performed in 70 (46.1%) of patients, subtotal thyroidectomy in 45 (29.6%) and lobectomy in 37 (24.3%) patients. The pathological diagnosis of all specimens removed is shown in Table 1.A total of 44 (29.0%) patients had their serum calcium decreased but remained within the normal range. Ten (6.6%) patients had TH and only four (2.6%) patients had PH. The incidence of TH and PH according to gender, age, type of operation, thyroid pathology, and inadvertent removal of parathyroid glands are shown in table 2. The four patients who developed PH were females who underwent total thyroidectomy. Two of them aged 42 years and the other two were elderly. One of them had thyroid cancer and the other three had multinodular goitre. Of the ten patients who had TH, eight were females, all were diagnosed as multinodular goitre, five underwent total thyroidectomy and five underwent subtotal thyroidectomy. The patients with TH had their serum Parathormone level decreased for a short period and then returned back to normal; meanwhile the four patients with PH had a sustained decrease in their serum Parathormone level. Inadvertent removal of parathyroid glands occurred in 10 (6.6%) patients. None of them developed PH and only one patient developed TH which resolved within few days. In three (30%) patients of cases with inadvertent removal of parathyroid glands the diagnosis of the thyroid disease was thyroid cancer and the operation was a second completion thyroidectomy in two of them with the parathyroid excision occurring in the second operation. The detailed features of these cases are shown in Table 3 Discussion Hypocalcaemia and injury to the recurrent laryngeal nerves are the most serious complications of thyroidectomy operation2. Although malignancy is the main indication for thyroidectomy operation, multinodular goitre is still the most common pathology for which thyroidectomy is performed. This is because of the cosmetic concern of some patients, the local pressure effect on upper respiratory and digestive passages and the possible association of malignancy with multinodular goitre9. In this study the pathology was multinodular goitre or other benign diseases of the thyroid in 137 (90.1%) patients and thyroid cancer in15 (9.9%) patients. This distribution of pathology is in agreement with that reported in the literature that shows that the most thyroid lesions that come to medical attention are benign and only 5-10% of them are thyroid carcinomas10 . Regarding our cancer patients although the total number of cases was small most of them (66.7%) were papillary carcinomas, a finding that is in agreement with other reported literature11 . Among those with multinodular goitre, 10% developed TH and 3% developed PH. All patients who developed TH and 75% of patients who developed PH had the diagnosis of multinodular goitre. One patient with thyroid cancer developed PH in whom the operation was total thyroidectomy . All cases of PH and TH occurred in patients following bilateral thyroid surgery [ total or subtotal thyroidectomy]. This finding is consistent with that reported in other studies that showed that the extent of resection and surgical technique has greater impact on the rate of post-thyroidectomy hypocalcemia than thyroid patholigical condition8, 12. Because the number of cases with TH or PH were small it was difficult to evaluate statistically the significance of the risk factors studied in the development of hypocalcaemia after thyroid operations. Inadvertent removal of parathyroid glands occurred in 6.6% patients. Of those, no one developed PH , one developed TH which resolved within few days. This finding is in agreement with others who reported an incidence of inadvertent parathyroid excision in the range of 6.415% and showed that such inadvertent parathyroid excision dose not cause a significant postthyroidectomy hypocalcemia13, 14, 15. In our patients with inadvertent parathyroid removal, three (30%) patients had thyroid cancer, eight (80%) patients had bilateral thyroid surgery and two (20%) patients had second completion thyroidectomy. These findings are in agreement with other studies which showed that thyroid cancer, extent of surgery and re operative surgery are risk factors for inadvertent parathyroid excision13, 14 . The slight decrease in postoperative calcium level in 44 (29%) patients could be due to haemodilution or minimal suppression of parathyroid function6. This should be evaluated more in a prospective study comparing thyroid and non-thyroid operations. None of our lobectomy patients developed post operative hypocalcemia but in two of them inadvertent parathyroid excision occurred. We calculated the incidence of hypocalcemia in both bilateral and unilateral thyroid operations because some of the lobectomies were associated with inadvertent parathyroid excision and assuming that the routine exploration of the other lobe adds a risk of trauma to the parathyroid glands in that side, in addition to the fact that some of the lobectomies were second completion operation. Excluding the lobectomy operations the incidence of TH and PH in this study will be 8.7% and 3.5% respectively. In this study the four patients who developed PH were females. In a retrospective study of 265 patients, Aboud et al8. found in a univariate analysis that female gender is significantly predictive of post operative hypocalcemia (p=0.0028). In the multivariate analysis of the same study it was not an independent risk factor.Thomusch et al12 in a multivariate analysis of 5846 consecutive patients showed that female gender was an independent risk factor for TH but not for PH. The gender difference in the development of post-thyroidectomy hypocalcemia remains an interesting subject for further prospective studies. This study may be limited by the sample size and the small number of patients who developed hypocalcaemia so the statistical significance of the risk factors studied could not be evaluated. Conclusion The incidence of post-thyroidectomy hypocalcaemia is low. It is seen only after bilateral thyroid surgery and is related to the extent of thyroid resection. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09005t2.jpg] [js09005t1.jpg] [js09005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}