 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
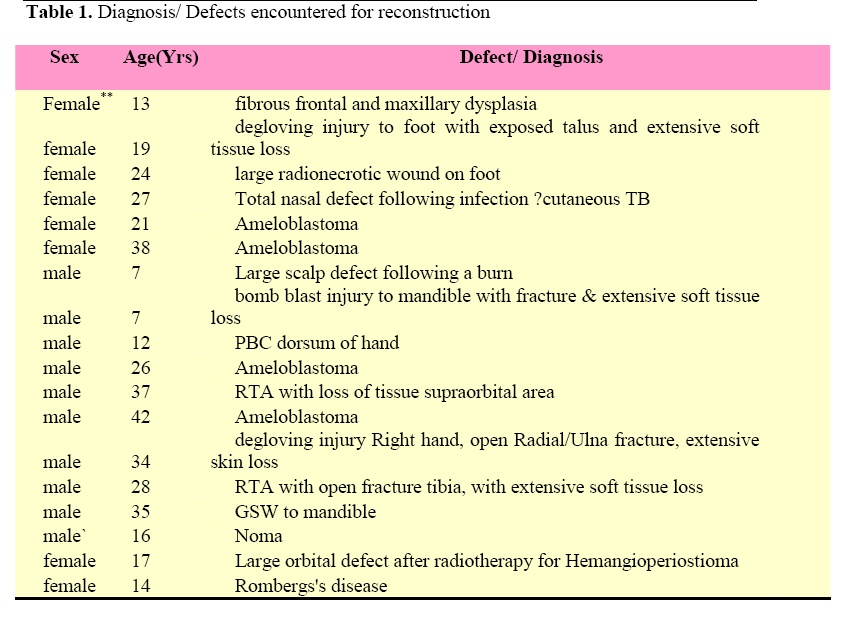
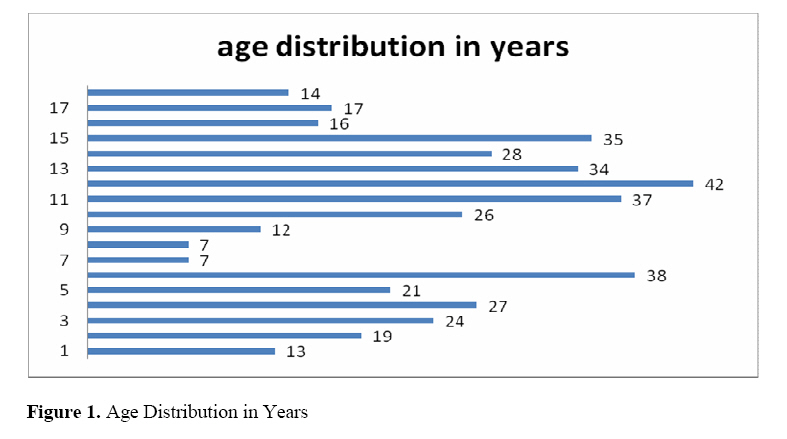
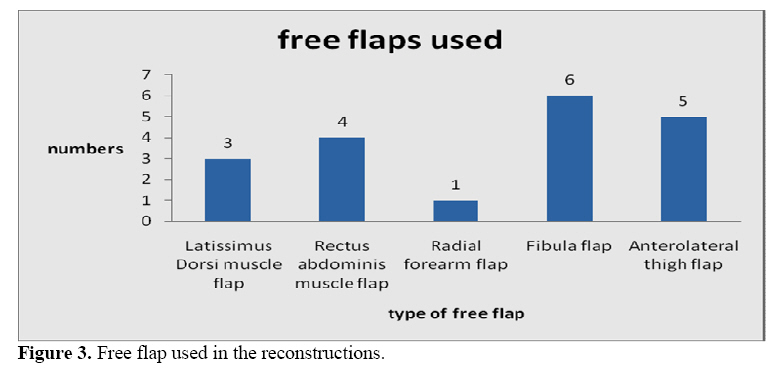
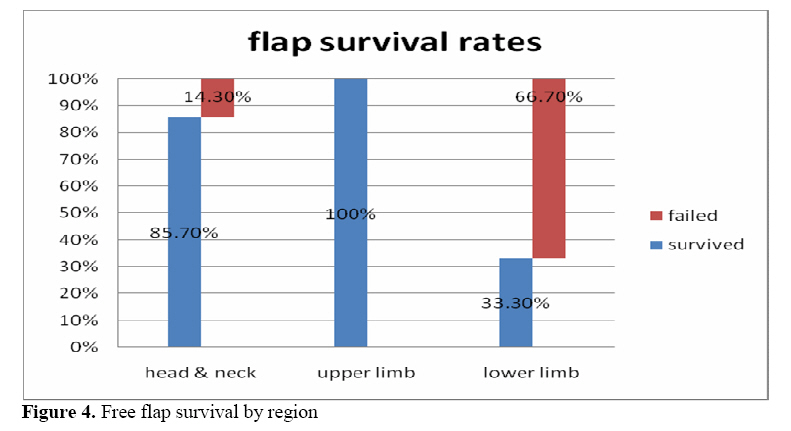
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 38-43 Free Flap Surgery at Mengo Hospital, Uganda -A Review of The First 19 Consecutive Microvascular Free Tissue Transfers. G.W. Galiwango Mengo Hospital, Kampala -Uganda. Code Number: js09006 Background: Microvascular free tissue transfer is an important method for reconstructing complex surgical and traumatic defects, allowing single stage reconstruction in most instances. This study reviews the first 19 consecutive free tissue transfer (free flap) reconstructions at Mengo hospital, Department of Plastic and Reconstructive surgery. Introduction Some defects created by trauma or following surgical excision of tumors require large volumes of tissue or composite tissues which are necessary to cover vital structures exposed in a wound, give functional and acceptable aesthetic results. To achieve a reconstruction that provides good soft tissue and vital structures cover, volume to fill a defect, allow acceptable or even nearly preinjury functional state and to give an acceptable aesthetic result can be a challenge to the trauma and cancer surgeon. Within the specialty of Plastic Surgery, many techniques have been developed to reconstruct large defects. These techniques involve using tissue such as skin, fascia, muscle or bone in reconstructions of various parts of the body for defects in tissue, form or function. For improved tissue survival and maintenance of its form and function, the tissue is raised with its vascular pedicle. This tissue may be raised from areas in proximity to the defect, in which case a pedicled flap1 is employed. However, if this is not possible for some reason e.g. local tissue is not desired or is insufficient; tissue can be raised with its blood supply from a more favourable site with little morbidity to the donor site and patient. A free flap is tissue (skin only, muscle with skin, muscle only or bone or digit transfers) transferred from a distant location on the body on its vascular pedicle and the blood supply reestablished by anastomosis to appropriately sized vessels at the recipient location; a process requiring microsurgical skills and appropriate equipment. The first successful free flap performed in the world was a free groin flap performed by Daniel and Taylor in 1973. Reconstruction with free flaps is nearly a novel technique used in surgical reconstruction in Uganda. From the records, the first successful microvascular free tissue transfer operation was performed in Uganda was in June 2005; a free Latissimus Dorsi flap was used to cover a 60% exposed skull following a burn on a 7 yr old boy ‘s head. This is a review of the first consecutive free tissue transfers performed at Mengo hospital from 2005 to date. Methods The clinical notes for all the patients that had surgical reconstructions using free flaps in Dept of Plastic & Reconstructive Surgery – CORU, Mengo Hospital, Kampala -Uganda from June 2005 to December 2007 were reviewed. Data collected included: sex and ages of the patients, area of reconstruction, flap used in reconstruction, duration of stay in hospital and outcomes. Results Nineteen surgical reconstructions using free flaps were found and reviewed (18 patients-one patient has had two free flaps reconstructions). This represented only 0.006% of the total procedures (3244) performed by the plastic surgical team over the period of time. Eight females and 10 males had microsurgical free tissue transfer reconstructions in this period (Table 1). Nineteen reconstructions with free flaps for defects in the head and neck, upper limb and the lower limb were performed during the period July 2005 to December 2007. Figure 1 shows the age distribution. Areas reconstructed included head and neck (73.6%); upper limb 10.5%) and lower limb (15.9%) (Figure 2). The head and neck defects included defects following excisions of fibrous dysplasia of the maxillary and frontal sinuses(n=1), supra orbital soft tissue loss following trauma(n=1), orbital exenteration with radionecrosis for Hemangiopericytoma(n=1), extensive scalp loss from burns,(n=1) extensive soft tissue loss and fractured mandible following bomb blast injury(n=1), mandibular excisions for ameloblastoma(n=4), noma(n=1), partial amputation of nose(n=1) and Romberg’s disease(n=1). The upper limb reconstructions were those for covering exposed extensor tendons after contracture release for severe post burn contracture of the hand (n=1) and an extensive degloving injury of the forearm with exposed nerves, tendons and fractured radius and ulna(n=1). The lower limb reconstructions included cover of exposed metatarsals and tendons following a degloving injury of the sole of the foot(n=1), cover of exposed ankle joint following chronic radionecrotic ulcer(n=1) and a Gustillo IIIB* injury following trauma(n=1). Choice of the tissue for free microvascular transfers performed was made after assessment of the area to be reconstructed in terms of what was missing/lost, were the missing structures replaceable by autogenous tissue, the functional and aesthetic outcome as well as assessment the donor area in terms of expendability of the tissues, resultant morbidity of the donor area, functional properties of the tissue to be transferred. Surgical details Informed consent for the surgical reconstruction involving the free tissue transfer was obtained. Preoperative co-morbidity was scored according to the American Society of Anesthesiology scale; all 19 patients were in class 1. Planning involved discussion of the options and planning of the flap as well as the procedure. The flaps were designed to avoid the need for vein grafts. All operations reviewed were performed in Mengo hospital plastic surgery unit. The core surgical, anaesthetic, theatre and nursing team was maintained for all the operations. Equipment used included a microvascular set with micro-vascular surgical instruments, an operating microscope (Zeiss Quadrascope™). A two team approach for tumour resection or recipient site preparation and flap raising was used whenever possible. Microvascular anastomoses were performed to vessels using both the interrupted (triangulation) and a continuous suture technique; end-to-end anastomoses were preferred. No systemic anti coagulant was used; however, HepSal solution 1:10000 was used to flush the vessels ends during anastomosis. Ambient temperature in the theatre was maintained at about 25 degrees Celsius. Surgery for each case lasted between 3 and 6 hours. Figure 3 shows the free flaps used in the reconstruction. Postoperatively, the condition of the flap was monitored by the surgeons using skin paddle warmth, color, texture or turgor, pin prick test, and Doppler on the flap along the axial direction of flow of blood along the vascular pedicle or a Doppler signal of good strength over the perforator supplying the flap. The duration of hospital stay ranged from 5 to 28 days with a mean of 11.3 and a median of 8 days. Fourteen free flaps survived; 10 of these were without incident and had uneventful post operative stay in hospital. Twelve (85.7%) of the 14 Head and Neck flaps, 2 out of 2 Upper limb and 1 out of 3 Lower limb flaps survived.(Figure 4). Complications were considered as perioperative if they occurred within 4 weeks of the operation. These included: 1; No reflow phenomenon: 2; Venous congestion: 1 -flap was inset into an orbital defect and with postoperative flap edema, suffered congestion overnight and by morning the flap was severely compromised and was not salvaged by loosening the insetting stitches; another patient, with the pedicle going across the cheek and the anastomosis to the facial artery and vein assumed a resting position against the pedicle a week after discharge from hospital leading to flap death. 3; wound break down occurred in 3 of the patients who had free fibula flaps for mandibular reconstructions. Of these, two settled after a course of antibiotics while in hospital and eventual resuturing. The other had wound break down after discharge. There were no deaths. Four (4) free flaps failed. These included: a free Rectus Abdominis flap to reconstruct a defect of the maxillary area caused by fibrous dysplasia; a free Rectus Abdominis flap providing soft tissue cover to a deep radionecrotic ulcer on the leg; a free Antero-lateral thigh flap to give soft tissue filing to a degloved supraorbital area; a free Latissimus Dorsi flap giving soft tissue cover to in a Gustillo type 3 wound of the lower limb defect. None of the patients with the failed flaps were returned to theatre in an attempt to salvage the flaps. Discussion Microvascular free tissue transfer is very demanding in terms of skill required of the surgical team as well as the anaesthetic and nursing teams, the complexity of the reconstructions undertaken and the stress of the length of surgery. Surgeons need to have skills in microvascular surgery and regularly practise as the learning curve is quite steep. However, it is very rewarding in that, defects otherwise thought of as un-reconstructable can be reconstructed. Free flap surgery allows both functional and aesthetic that would otherwise be difficult to achieve with other methods of reconstruction. Some defects following tumour excision or trauma involve extensive loss of soft tissues and other times bone. Some of these defects are not amenable to traditional methods of reconstruction e.g. cover for large soft tissue defects, osseous reconstructions with autologous bone. A failure rate is invariably observed with free tissue transfer. The failure rate observed in this series is higher than what is quoted in series from centres in the more developed countries; this however can be reduced to even such levels as seen in more experienced centres. Increase in numbers of free tissue reconstructions undertaken and reliance on some flaps for particular reconstructions and a two team approach will help reduce the failure rates as would a well drilled and dedicated team. Considering the defects being reconstructed and the duration of surgery as well as its complexity, the duration of hospitalisation shortened, and with a successful flap transfer, the patient is soon ambulant and is discharged after a few days frequently not requiring more major surgery thereafter. Increased interdisciplinary consultations on surgical cases requiring complex reconstructions should be encouraged as this will improved surgical outcomes for the patients in terms of function and aesthetics. General and detailed understanding of microvascular free tissue transfer by the surgical, anaesthetic and nursing teams is essential to the smooth running and eventual success of the operation. The more free flaps performed, the better the team gets. Hopefully, the next 20 cases will have a much reduced failure rate. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09006f4.jpg] [js09006f1.jpg] [js09006f2.jpg] [js09006f3.jpg] [js09006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}