 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
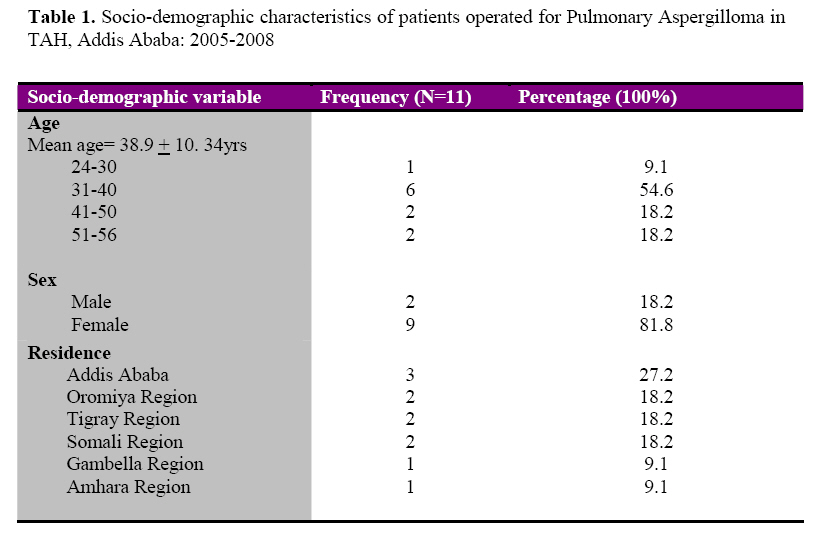
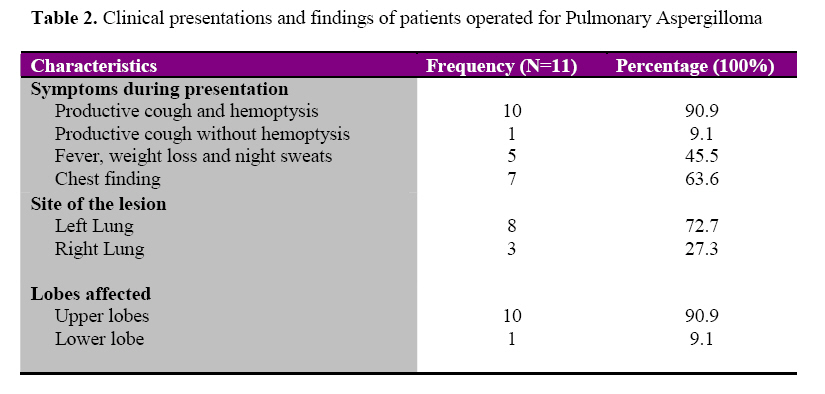
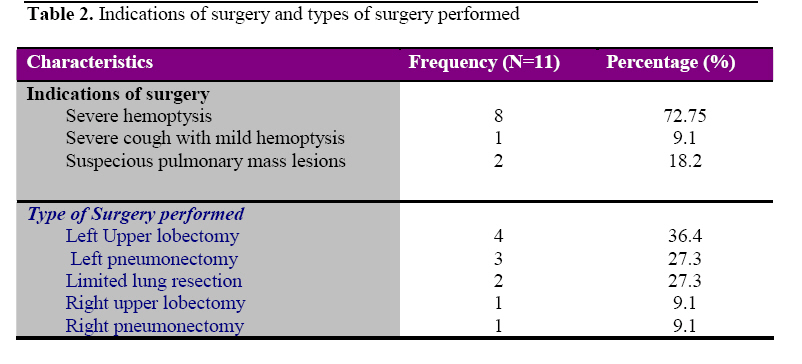
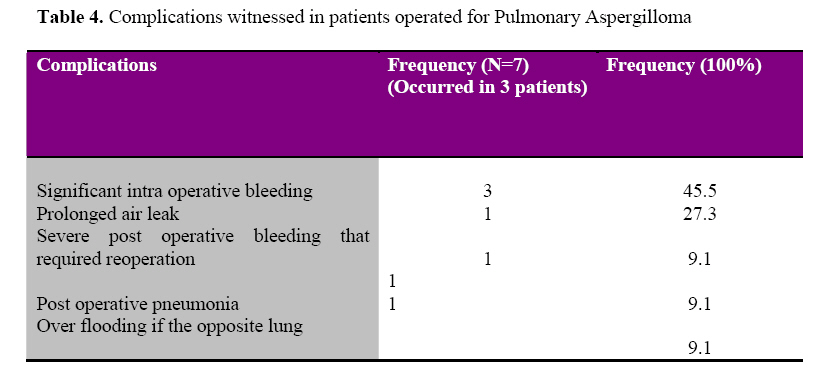
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 44-49 Aspergilloma of the Lungs: Operative experience from Tikur Anbessa Hospital, Ethiopia A. Bekele, D. Gulilat, S. Kassa, A. Ali Department of Surgery, Addis Ababa University, Faculty of Medicine Code Number: js09007 Background: Pulmonary aspergilloma represents a potentially life-threatening disease caused by saprophytic growth of Aspergillus fumigates in pulmonary cavities. This is the first report of its operative treatment from Ethiopia.The aim of this study was to determine the clinical presentations, operative treatments and post operative outcome of patients with pulmonary aspergilloma. Introduction Pulmonary infections caused by the fungus Aspergillus can occur in varying clinical forms i.e. aspergilloma, allergic broncho-pulmonary aspergillosis or invasive/semi-invasive aspergillosis1. Aspergilloma represents a potentially life-threatening disease caused by saprophytic growth of Aspergillus fumigates in pulmonary cavities and is usually located in the upper lobes of the lungs to form a fungal ball or mycetoma2,3. The fungal ball is made up of a tangled mass of fungal hyphae, fibrin, epithelial cells, mucus, debris and blood cells4. Fungal pulmonary colonization usually occurs after super-infection of pre-existing pulmonary cavities from previous chronic lung diseases such as tuberculosis, bronchiectasis, cavitating carcinoma, sarcoidosis, histoplasmosis bronchogenic cyst or chronic lung abscess5,6. In a study of 544 patients with pulmonary cavities secondary to tuberculosis, 11% had radiologic evidence of aspergilloma6 and according to a large survey conducted by British Tuberculosis Association, it occurred in 12% of healed tuberculosis patients7. Patients with aspergilloma should undergo surgical treatment, because there is a risk of sudden life threatening hemoptysis and because there is no effective alternate medical therapy5. Surgery offers the only realistic chance of a permanent cure and it very effective in prevention of recurrence of hemoptysis. Some authorities recommend early surgical resection of symptomatic aspergilloma and even in asymptomatic cases5,6,7. Pulmonary aspergilloma is not uncommon in Ethiopia. From 26 patients operated for complicated pulmonary tuberculosis at the same center over a period of 5 years, 27% of the surgeries were for pulmonary aspergilloma8. This is the first published report from Ethiopia that described the patterns of patients with pulmonary aspergilloma who were surgically treated surgically. Patients and Methods During a three-year period (April 2005-March 2008), 11 patients were admitted and operated on at the Tikur Anbessa Hospital (TAH) in Addis Ababa, Ethiopia, Chest Surgery Unit for pulmonary aspergilloma. The patients’ records were retrieved and data concerning their sociodemography, presenting symptoms and findings, imaging studies, intra-operative findings, operative procedures, post operative course and final out comes were collected. After data collection, analysis was done using computer based statistical software EP-INFO-2002. Overall, 11 surgical procedures were carried out. Routinely, these patients were initially evaluated and treated by chest physicians and then referred for surgery. Decision to operate was reached after joint discussion between the chest surgeons and physicians. All patients were operated under general anesthesia and with double lumen endo-tracheal tubes in situ for adequate isolation and selective ventilation, through standard postero-lateral thoracotomy. Considerable adhesions were seen in all of the cases and significant bleeding occurred in most. Post-operative, patients were transferred to the Surgical ICU and then to their regular wards when their condition stabilized. Mechanical ventilation was employed for a limited period in patients who couldn’t maintain their breathing on their own. All operative specimens were sent for histopathologic study. However, fungal culture was not done. Results During the study period, 11 patients were admitted for surgical treatment of pulmonary aspergilloma, 81.8% of these patients were males. Their ages ranged from 24 to 56 years (Mean=38.9 and Median=35 years). Most were in their third and fourth decades (72.8%). They came from all over the different regions of the country (Table 1). The mean duration of illness before admission was 16.9 months (Lowest=6 months, highest=36 months). Cough and hemoptysis were the two most common presenting symptoms, occurring in 11(100%) and 10(90.9%). The constitutional symptoms of tuberculosis such as low-grade fever, weight loss and night sweats were reported by 5(45.5%). Eight patients completed standard short course anti-TB medications twice and three were still taking their first course. All received different courses of antibiotic therapy for variable duration before surgery. All patients were negative for HIV infection and none had evidence for immune-suppression. Ten (90.9%) were clinically malnourished. The chest x-ray features revealed cavitary lung lesion in 5(45.5%), typical features of pulmonary aspergilloma in 4(36.4%) and a suspicious solid pulmonary mass lesion in 2(18.2%). Chest CT-Scan was done for three patients and it was diagnostic of aspergilloma in two and it was suspicious for pulmonary neoplasm in one. The left lung was involved in 8(72.75%) and the right side in 3(27.3%). The upper lobes were the most commonly affected lobes occurring in 10 (90.9%) and the lower lobe in 1(9.9%). All were solitary lesions (Table 2). The most frequent clinical indications for surgery were severe haemoptysis in 8 (72.75%), suspicious lung carcinoma in 2(18.2%) and severe cough with mild hemoptysis in 1(9.1%). Pre-operatively, all patients were put on anti-TB drugs, some were started on antibiotics and adequate chest physiotherapy delivered. No patient was put on any form of anti-fungal treatment. The performed procedure were left upper lobectomy in 4(36.4%), left pneumonectomy in 3(27.3%), limited resection of the upper lobes in the right side 1(9.1%) and the left 1(9.1%), right upper lobectomy in 1(9.1%) and right pneumonectomy in 1(9.1%). (Table 3). All surgeries were accompanied by bleeding of 750ml. of blood and three (27.3%) procedures were associated with bleeding of more than 2 liters. Intra-operative injury to major bronchus occurred during 1(9.1%) procedure. Four significant complications occurred in the postoperative period. These include prolonged air leak for more than 20 days (1), severe post operative bleeding that required reoperation (1), post operative pneumonia (1), and over flooding of the opposite lung during extubation (1). The prolonged air leak after a right pneumonectomy responded to prolonged chest tube drainage, the patients with significant post operative bleeding had to be re-explored after 6 hours of surgery to control the bleeding from a major bleeding vessel and the post operative pneumonia responded to antibiotics and chest physiotherapy. However, the patient who developed severe contamination of the healthy lung during extubation died on the 4th post operative day due to severe respiratory failure, making the postoperative mortality 9.1%. All the ten patients who were discharged improved were followed up for 6 months and all are symptom free. Histopathologic confirmation of the fungal ball was possible in all 10 patients, the underlying disease identified to be tuberculosis in 9(90%) and bronchiectasis in 1(10%). Discussion During the three-year period, surgery for pulmonary aspergilloma accounted for 5.8% of all thoracotomies done at the hospital. Eleven cases seen over three years in a national referral hospital (average of 3.6 patients per year) in a country where tuberculosis is very rampant might give the impression that aspergilloma is a rare disease. However, we believe this is the tip of the ice berg and many asymptomatic and undiagnosed patients might be still out there. Aspergilloma in Ethiopia doesn’t seem to cluster in particular areas of the country since we have seen that the patients came from all over the country. In our series, the commonest lung pathology behind the aspergillus lesions was cavitary pulmonary tuberculosis. This is reported from other African and Asian reports but different from a German report which states that bronchiectasis is the most common underlying pathology16 . Aspergillomas predominantly occurs in the upper lobes, and on the left side. Literature review also shows that this is due to the fact that the upper lobes are prone for cavity formation at the relative imbalance in perfusion and ventilation in the apices, which provides an oxygen-rich environment for invading organisms3,4,5 . Generally, reports state that patients present with significant hemoptysis and chronic productive cough, which can be life threatening7,9 . This was also found to be true in our patients. Radiologically, aspergilloma typically is evident as an upper-lobe, mobile, intra-cavitary mass with an air crescent in the periphery and the adjacent pleura may be thickened9,13. In our case, it was in only 4(36.4%) that this typical feature was present. However, at times, the mass might not be easily seen on routine chest radiograph. This occurred in 5(45.5%) of our patients where the cavitary lung lesion was predominantly visualized and two x/rays were suspicious for solid lung neoplasms. It is said that chest CT scan may be necessary to make an accurate diagnosis in such cases10,13 . However, in developing countries like as Ethiopia, the affordability and routine availability of CT scan is a serious issue. It is worth remembering that aspergilloma usually complicates pulmonary tuberculosis, which intern predominantly occurs in the economically deprived societies. Therefore, we believe that chest x/ray is sufficient enough an investigation to decide on early surgery in patients who present with suggestive symptoms. A definitive diagnosis of pulmonary aspergilloma can be made after histopathologic examination or culture of the resected specimen. We have found that histopathology is practical since the diagnosis in all our patients was confirmed the same way. However, we didn’t routinely do fungal cultures. Isolation of the fungus from sputum is possible but its sensitivity is low given frequent non-pathologic airway colonization4. Serological diagnosis has reasonably good sensitivity and specificity but has limited clinical importance in a typical scenario. However, we haven’t utilized serology in our patients and we believe that this is a room for improvement. In our center, we have adopted the policy of early surgical treatment for all cases with aspergilloma. The literature also supports that surgery is the best option of treatment. According to some authors, successful treatment of complex aspergilloma needs both surgery and perioperative anti-fungal chemotherapy. Amphotericin B, 5–flucytosine, Itraconazole and most recently caspofungin had been utilized and some degree of response has been reported4,11,12 . Other therapies include intra-cavitary instillation of antifungal agents and embolization of bronchial arteries for hemorrhage. It has also been reported that approximately 10% of aspergillomas spontaneously resolve13 . Surgery for pulmonary aspergilloma has been the standard in many centers, but can be associated with high morbidity and mortality7,9 . The underlying significant pulmonary pathology, the immune status of the patient, malnutrition, and the presence of significant adhesions that make the operative procedures difficult might be related to the complications such as bleeding, residual pleural space, broncho-pulmonary fistula, empyema, and respiratory failure. The mortality from surgery for aspergilloma is reported in the ranges between 7% and 23%7,8,9,10. In our series, the mortality was 9.1%, well in range with those reported by others 10,14,15 . Conclusion
References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09007t2.jpg] [js09007t3.jpg] [js09007t1.jpg] [js09007t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}