 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 57-63 Head Injury at a Tertiary Referral Centre in the Eastern Region of Nepal. A. Agrawal , C.S.Agrawal, A. Kumar, O. Lewis, G. Malla, P. Chalise 1Consultant Neurosurgeon, Department of Surgery, B.P. Koirala Institute of Health Sciences, Code Number: js09009 Background: The purpose of this epidemiologic study was to determine the pattern and characteristics of head injuries and to establish an epidemiologic data bank for designing preventive strategies for head injuries in the eastern region of Nepal. Introduction Head injuries are one of the leading causes of death and disability worldwide1,2,3 . Although many head injuries are minor, because of the devastating effects of moderate and severe head injuries, they constitute an important public health problem. In order to prevent head injuries there is a need to identify causes, especially with regard to motor-vehicle crashes, and to implement strategies to reduce their occurrence. The purpose of this epidemiologic study was to find out the pattern and characteristics of head injuries and to establish an epidemiologic data bank for designing preventive strategies for head injuries in the eastern region of Nepal. Materials and Methods This retrospective review was performed at B.P.Koirala institute of Health Sciences, Dharan, Nepal. All of the patients with head injury admitted to the Department of Surgery between the periods January 2005 to December 2005 were reviewed. All clinical records, investigations and treatment charts were reviewed. Age, gender, etiology and pattern of injuries, anatomic site of cranial lesions, associated systemic injuries, treatment details, complications and outcome were noted and analyzed. The Ommaya classification of head injury was used and patients with head injuries were categorized into three grades; mild, moderate, or severe categories (based on the period of loss of consciousness and amnesia)4. Neurological injuries ranged from loss of consciousness to depressed skull fracture requiring neurosurgical intervention. Systemic injuries were grouped into following categories:
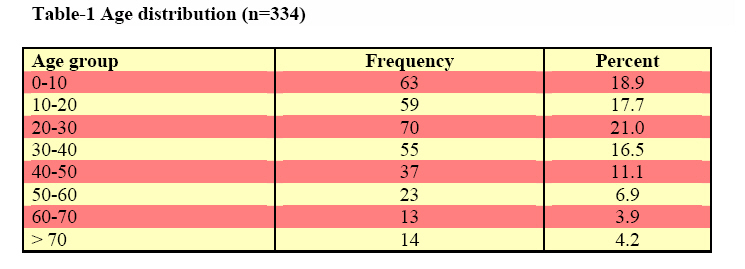
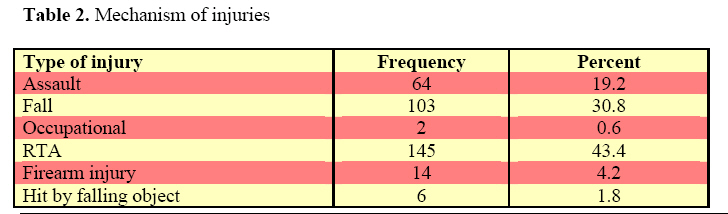
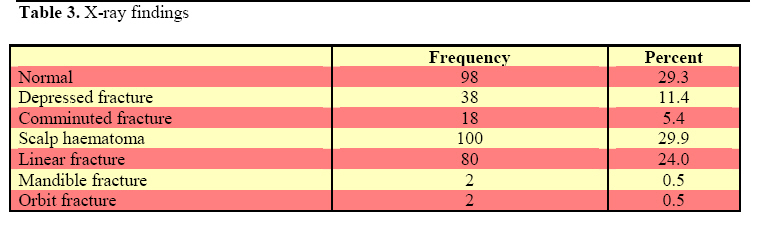
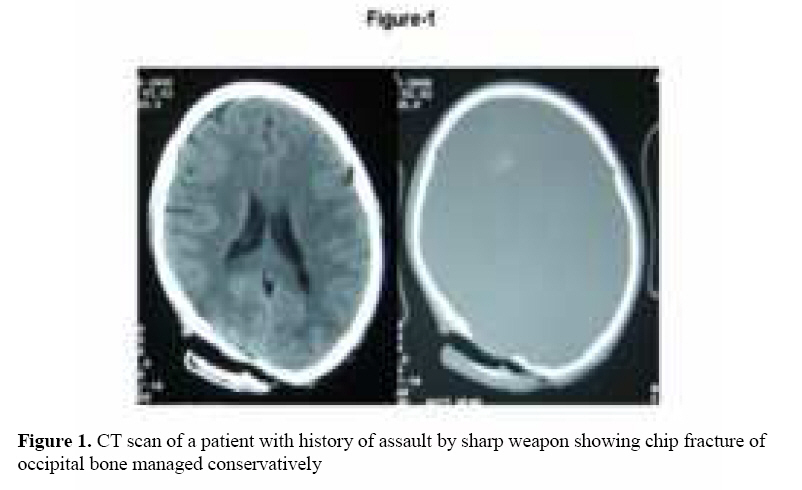
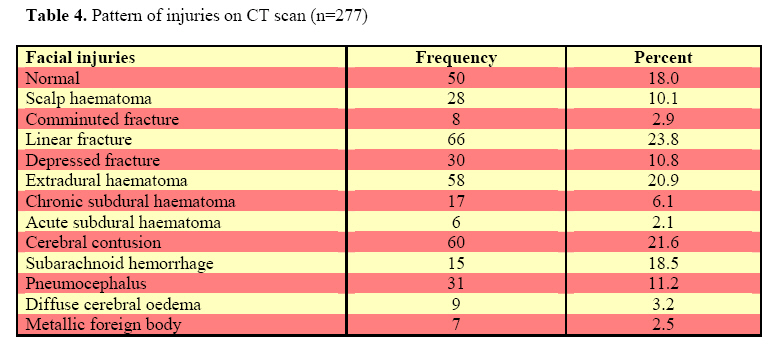
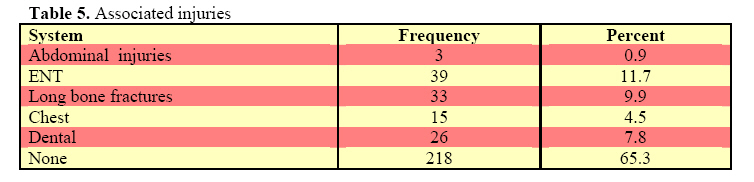
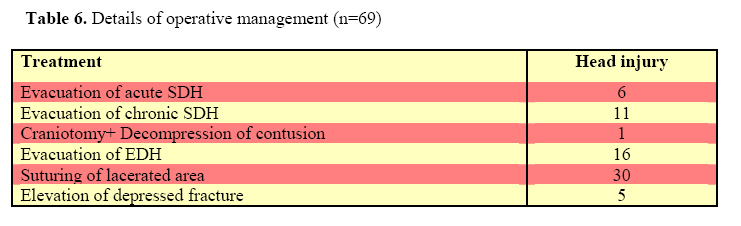
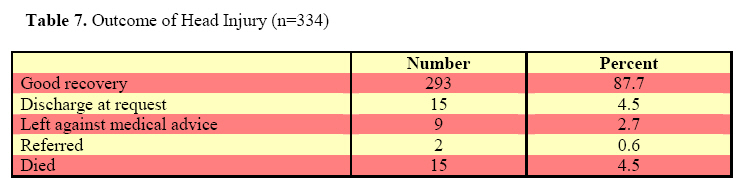
Results There were total 334 patients in present study who sustained head injuries. In present study majority of the patients were young adults 2nd to 5th decade (66.3%). Also in the present study there was high incidence of head injuries in the 1st decade of life (18.9%). Patients after 50 years (15%) were less commonly affected (Table 1). Mean age was 28.53 years (range 1 to 88 years). There was predominance of males (71.9 %) in our study. The male to female sex ratio was 2.56:1. Road traffic crushes were the commonest causes of head injuries in present study (43.4%) followed by fall from height (30.8%), assault (19.2%) and firearm injuries (4.2%). Falling object (1.8%) and occupational injuries (0.6%) were less common causes of head injuries (Table 2). X-rays were performed in all the cases and findings are shown in Table 3. It was normal in 98 (29.3%) cases and showed scalp haematoma in 100 (29.9%) cases. X-ray skull showed lesions in 114 cases (49.8%), depressed fracture (11.4%), comminuted fracture (5.4%), linear fracture (24.0%), mandible fracture (0.5%) and orbit fracture in 2 (0.5%) cases respectively. CT scan was performed in 227 cases and it showed single lesion in 150 cases, two lesions in 57 cases and multiple lesions in 29 cases (Figure 1). CT scan was normal in 50 (18.0%), and showed one lesion in 150 (54.2%), two in 57 (20.6%) and three lesions in 20 (7.2%) of the cases. Common lesions on CT scan (Table 4) were cerebral contusion (21.6%), extradural haematoma (20.9%), linear fracture (23.8%), subarachnoid haemorrhage (18.5%), depressed fracture (10.8%) and pnemocephalus (11.2%). Comminuted fracture (2.9%), diffuse cerebral oedema (3.2%), acute subdural haematoma (2.1%) and chronic subural haematoma were less common lesions. There was presence of metallic foreign body in 7 cases (3.2%). Most of the patients (71.6%) sustained mild head injury, 40 (12.0%) sustained moderate head injury and 16.55% had severe head injury. Majority of the patients (79.0%) did not have any neurological deficits, only seventy patients (21.0%) had neurological deficits. Nasal or ear bleed was observed in 11.7% of the cases. A total of 59 patients (34.7%) had associated injuries (Table 5). Long bone fractures were seen in 9.9%, dental injuries in 7.8% and chest injuries in 4.5%. Only three patients (0.9%) sustained abdominal injuries. Out of 334 patients 39 patients (11.7%) required some form of surgical intervention. The majority (88.3%) of the patients was managed conservatively. Majority of patients had mild head injury and treated conservatively in present series. In thirty three patients suturing of lacerated scalp wound was performed. 16 patients underwent surgery for the evacuation of extradural haematoma, 11 patients underwent evacuation of chronic subdural haematoma, 6 patients underwent evacuation of acute subdural haematoma and in one patient evacuation of contusion was performed (Table 6). Majority of the patients (87.7%) made good recovery. Six patient developed wound infection and were treated conservatively. Fifteen (4.5%) of patients died in this series. One patient had associated intra-abdominal injury (splenic rupture) and two patient sustained pulmonary trauma and succumbed to haemothorax and aspiration (Table 7). Discussion There were total 334 patients in present study who sustained head injuries. In present study young adult males were commonly sustained head injuries. In literature also the vast majority of head injuries are experienced by males and young adults. 5, 6, 7,8,9,10,11 71.9 % of patients in our study were male and incidence of head injuries in female was 28.1 percent (male to female ratio2.56:1). These findings are consistent with previous studies also overall ratios of males to females have ranged from 3:1 to as high as 11.1:1 in literature. 5,8,10,11 High risk of head injuries in male gender may be due because males younger than 3 years have less freedom and mobility to engage in risk-taking activities or are less likely to have risk-taking behavior. They are also more vulnerable to bite and fall injuries. 12 Road traffic crushes were the commonest cause of head injuries in most of the series as supported by the present study. 5, 12, 13, 14 This may be attributed to recklessness and negligence of the driver, poor maintenance of vehicles, often driving under the influence of alcohol or drugs and complete disregard of traffic laws. 8 Fall as a common cause of head injuries may be due location of the hospital in Himalayan foothills. Fall is an uncommon cause of head injuries in the literature. 8, 15 Assault was also a common cause of head injuries in the present series and it may be due to the high incidence of interpersonal violence in this area. Interpersonal violence, especially the use of fists, is found to be the leading cause of trauma. However due to underreporting by patients, sometimes the correct incidence may not be possible. 5 Incidence of associated injuries was low in comparison to the literature where a large proportion of patients (35%) had associated injuries, such as abdominal, chest, and limb fracture injuries. 12, 16 Head trauma can affect skull, brain, and its meninges. High velocity impacts result in ruptures of intracranial vessels, leading to hemorrhages in different compartments. These accompanying injuries can be more life-threatening than simple injuries.17,18,19,20 In present series almost 50% patients had normal X-rays and remaining patients had associated fractures. However X-rays can not demonstrate associated intracranial injuries. CT scan was more useful in demonstrating the intracranial lesions. As in the present series most of the injuries are minor in nature and can be treated conservative. Even majority of the lesions on CT scan do not require neurosurgical intervention1,2,3,21,22,23 . Causes of surgical intervention for intracranial lesions in present series were compound depressed fractures, decompression of contusion, and evacuation of intracranial haematomas and suturing of scalp lacerations. 24 Six patient developed wound infection and these were treated conservatively. Fifteen patients were expired in this series. One patient had associated intra-abdominal injury (splenic rupture) and other patient sustained pulmonary trauma and succumbed to haemothorax and aspiration15,25,26 . The major cause of mortality in this review was severe head injury. 27 Because this was a retrospective review and the information was obtained by chart review, it relies on the accuracy of both the history provided and the history recorded. In some cases, the information was provided by witnesses to the events; however, in other cases it was provided by the patient. Additionally, the history was recorded by different health care providers in nonuniform fashion. The above data work on the assumption that the history is an accurate representation of the events that transpired. Ideally, the investigators would perform all history taken and use a standard methodology in history taking to better ensure accuracy regarding data. Conclusions Road traffic accidents were the commonest cause of head injuries, young patients were most commonly affected in present study with a male preponderance. This study will provide a clearer understanding of the patterns of head injuries and will assist health care providers to plan and manage the treatment of traumatic head injuries. This epidemiological information can also be used to guide the future funding of public health programs geared toward prevention. In this study we analyze epidemiology, clinical characteristics and management options in patients with head injuries in a tertiary referral centre of Eastern Nepal. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09009t6.jpg] [js09009f1.jpg] [js09009t3.jpg] [js09009t2.jpg] [js09009t4.jpg] [js09009t7.jpg] [js09009t5.jpg] [js09009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}