 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
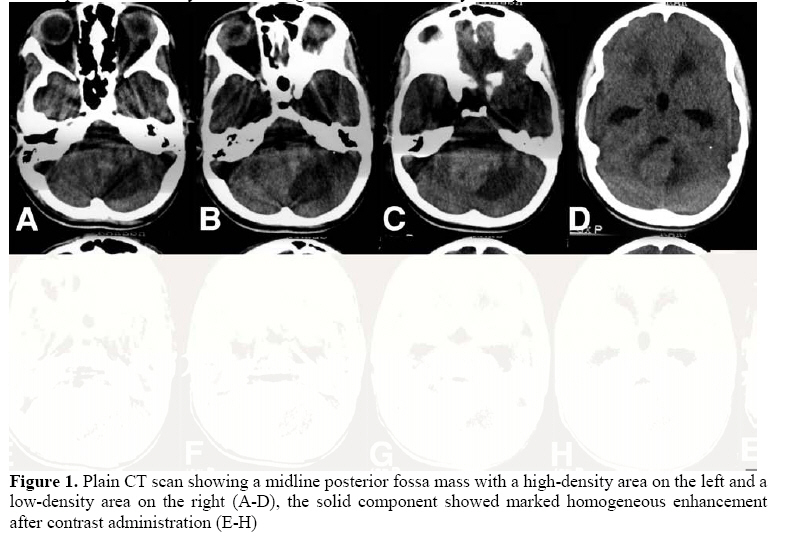
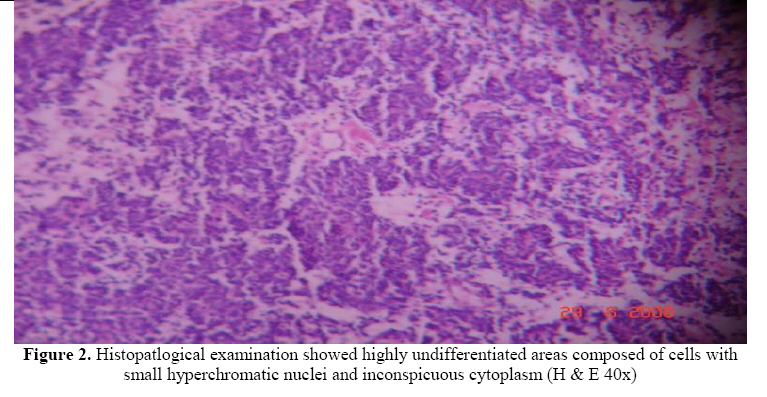
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 73-75 Cystic Medulloblastoma in a child A. Agrawal1, A. Agrawal2, D.N. Balpande3, C.S. Pathak3 1Associate Professor in Neurosurgery, 2Associate Professor in Pathology, 3Professor in Pediatrics, Code Number: js09012 Introduction Medulloblastoma is a commonly encountered, highly malignant posterior fossa midline cerebellar tumour of children, with a tendency to early recurrence and dissemination through the cerebrospinal fluid1-8 . On computed tomography, majority of the medulloblastomas have a typical appearance, consisting of a mass of uniformly increased density that enhances homogeneously after contrast enhancement with sharp demarcation of the neoplasm and there may be associated hydrocephalus2-8 . Case Report This 14 year male child presented with headache, vomiting and swaying while walking to either side of 1 month duration and loss of vision of 15 days duration. On examination, the child was conscious and well oriented. He had bilateral papilloedema. There was no perception of light or projection of rays in both the eyes. Eye movements were normal and he had bilateral cerebellar signs. There were no other neurological deficits. CT scan (Figure-1) showed a mass in the midline of the posterior fossa, comprising a solid isodense component on the right and a cystic hypodense component on the left, having a density slightly higher than cerebrospinal fluid. There was diffuse enhancement of the solid component. The fourth ventricle was compressed and displaced anteriorly and to the right with associated hydrocephalus. The child underwent midline suboccipital craniectomy, vermis was split, there was a big cyst containing xanthochromic fluid that was evacuated and the bulk of the grayish,, soft friable, highly vascular tumor was resected. Histopathological examination showed the tumor cells with poor cytoplasm, oval nuclei and formed Homer Wright rosettes (Figure-2). A diagnosis of cerebellar medulloblastoma was made. Following surgery he improved in his headache, vomiting and cerebellar signs but there was no improvement in his vision. He was subjected to cranio spinal irradiation and is on regular follow up with no fresh symptoms. Discussion Up to 47% patients of medulloblastoma can have atypical features on CT scan5 and these include cystic or necrotic component, calcification, hemorrhage, lack of contrast enhancement, eccentric location, rarely direct transtentorial extension5,9. Cystic or necrotic component is less common in children than in adults5,10-12. Presence of these atypical features on CT scan can make it difficult to differentiate a medulloblastoma from other posterior fossa tumors i.e. ependymoma and astrocytoma in children5. In a child is who have a central well-marginated tumor which exhibits uniformly increased density on pre-contrast scans and homogeneous contrast enhancement there is 85-90% likelihood it to be a medulloblastoma, 5 however the presence of atypical features on CT scan in the first decade of life should not be considered against the diagnosis of medulloblastoma. 5,9 References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09012t2.jpg] [js09012f2.jpg] [js09012t1.jpg] [js09012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}