 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
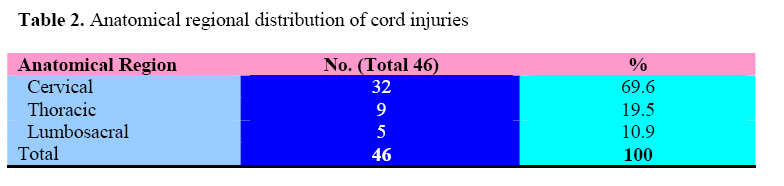
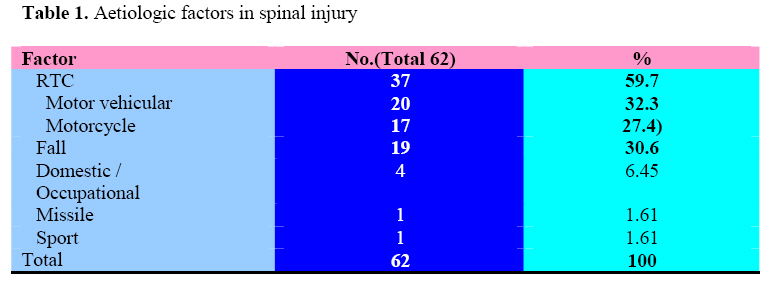
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 76-80 Patterns of spinal injury in a new neurosurgical centre: A 2-year prospective study J.K.C. Emejulu1, O.C. Ekweogwu1, Timothy Nottidge2 1Neurosurgery Unit, Department of Surgery, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria 2University of Uyo Teaching Hospital, Uyo, Akwa Ibom State, Nigeria Code Number: js09013 Background: Spinal injury is a major cause of morbidity and mortality worldwide. Road traffic accident is the main aetiologic factor, affecting mostly the male gender in the >15 – 40-year age group. The aim of this study was to establish our local hospital patterns of spinal injury and compare them with published reports. Introduction Spinal injury is trauma to the cord and/or its surrounding structures including the vertebral bones, ligaments and blood vessels as a result of an externally applied mechanical force, and aetiologic factors include road traffic accident, fall, missile, assault, domestic / industrial accident and sport / recreational activity1,2,3,4. This definition appears to differ slightly from the contentions of some workers like Green et al, who in specifically defining cord injury, went further to expand the aetiologic factors to include infection, tumor, vascular compromise, and degenerative disease5. In contradistinction to this concept, we do not regard non-traumatic assaults to the cord as spinal injury in our own service, just as we do not include them in head injury. Estimates indicate that 2:100,000 population per year are affected by spinal injury, and majority are aged 16 – 30years, with a male:female ratio of 4:16,1 . Spinal injuries could affect the neural and non-neural tissues simultaneously or independently, and there is no correlation between injuries to these different tissues8,9. The cervical region is the most frequently injured part of the spine (42-50%), followed by thoracic (31%) and lumbosacral (27%)10. About 50% of injuries result in quadriplegia, as neural injuries could affect the spinal nerves and/or spinal cord; the cord injuries could be complete or incomplete11. Complete injuries are regarded historically as the absence of normal sensation beyond two spinal levels from the point of injury, but the American Spinal Injury Association, ASIA scale regards all injuries without sensory preservation at the S4-5 dermatome as complete12,13,14. More than half of cord injuries are thought to be incomplete, mostly central cord syndrome, followed by anterior cord syndrome9,11,12 . Incomplete injuries are classified into 4 major syndromes, with occasional atypical combinations of these viz. anterior, posterior, lateral and central cord syndromes13,14,15,16 . Conus medullaris syndrome is more commonly associated with thoracolumbar injuries15,16 . Evaluation of spinal injuries is best done by imaging studies, and magnetic resonance imaging (MRI) is the gold standard with soft tissue injuries, whereas bony lesions are best investigated by computerized tomography (CT)17. Plain radiography is still useful in places where modern imaging is not readily available and could still find use in the evaluation of suspected vertebral injuries without neurological deficits. Treatment could be operative or non-operative depending on the clinical diagnosis of the primary and/or secondary assault, major indications for surgery being neural compression and bony instability18 . Outcome depends on the extent of neural injury, as patients with complete cord injuries appear not to make neurological recovery, and those with incomplete injuries have been reported to recover to various extents19,20,21 . In April 2006, neurosurgical services were commenced in our centre. We undertook a prospective study of spinal injury patients from that period in an attempt at establishing our local baseline epidemiological patterns and comparing them with published reports. Patients and Methods A prospective study of all spinal injury patients treated in our service in the two-year period, April 21, 2006 – April 20, 2008 was undertaken. Data collection was from the time of admission into our service to the time of discharge using a structured proforma, and subsequent follow-up in the few cases that kept to their appointment. Data was then collated and simple analysis done. Outcome was evaluated with the Frankel scale viz. A -complete loss of functions; B -sensory preservation without motor function; C -useless motor preservation; D -useful motor preservation; E -normal or near-normal function. Our centre is a tertiary health facility receiving referrals from several primary and secondary facilities all over our geopolitical zone and surrounding zones in Nigeria’s six-zone structure. Results Spinal injuries were diagnosed in 62 of the 826 patients seen in our neurosurgical unit within the 2-year period, representing 7.5% of all our consultations. There were 6(9.68%) aged 0-15years 28 (45.2%) in the 15-40years, 23 (37.1%) aged 40-60years 5 (8.1%) aged above 60years. Most 58(93.5%) of the patients were admitted through the Accident and Emergency Unit and the rest from the Surgical Out-patient Unit 3(4.84%) and Children’s Out-Patient Unit 1(1.6%). One patient was in her 2nd trimester of pregnancy at the time of injury. Males accounted for 47(75.8%) of the cases, giving a male: female ratio of 3.1:1. Road traffic crush was the aetiologic factor in 37(59.7%), fall 19(30.6%), domestic/occupational accident 4(6.45%), missile 1(1.61%) and sport 1(1.61%). Among the cases of road traffic accident, 20(32.3%) were motor vehicular and 17(27.4%) motorcycle, (table 2). There were neurological deficits in 49(79%) of the 62cases whereas 13(21%) had injuries without deficits; vertebral 10(16.1%) and soft tissue 3(4.84%). Cervical cord injuries were 32(51.6%), thoracic 9(14.5%) and lumbosacral 5(8.06%); with radiculopathy 3(4.84%), (table 3). There were 24(38.7%) complete, and 22(35.5%) incomplete cord injuries, with associated head injuries in 36(58.1%) and other systemic injuries 25(40.3%). Evaluation of the spinal injuries was with plain radiography 58(93.5%) and computerized tomography 3(4.84%); 4(6.45%) did not do requested imaging investigations. Among the cases with cervical cord injury 15(24.2%) had fractures and another 15(24.2%) had translocations (subluxations) without fractures, 2(3.23%) had cord injuries without radiological evidence of trauma, thereby necessitating computerized tomography. In the thoracic region, fractures were 4(6.45%) and subluxations 2(3.23%); and in the lumbosacral, subluxations were 3(4.84%) and fractures 2(3.23%). Treatment was non-operative in all cases with Gardner-Wells’ Tongs traction or rigid neck collar for cervical spinal injuries 32(51.6%), and postural reduction for the thoracic and lumbosacral injuries. At the time of discharge, all cases of complete cord injuries remained without neurological improvement, whereas 20(32.3%) of the 22 cases of incomplete cord injuries recorded varying degrees of neurological recovery. Mortality was 13(21%) and all had cervical cord injuries. Follow-up was mostly unsuccessful as only 19(30.6%) turned up after discharge from our Unit. Discussion Epidemiologically, the pattern of our cases correlated with other published reports with a preponderance of males, and most were aged >15 – 40 years6,1 . Our anatomical regional distribution of cord injuries tallies with universally reported patterns with the cervical cord mostly affected, followed by thoracic and then lumbosacral, but our aetiologic factors appear to be modified with quite a significant number (17 out of 37 incidents of RTA) caused by motorcycle accidents, unlike in other reports1,2,3,4 . Being a predominantly trading community with many bad road networks necessitating the preferential use of motorcycles over motor vehicles, and commuters ferrying men and materials, it was no surprise that road traffic accident was the leading causative factor. But, even though there were more incidents from motor vehicles as in other reports, with the motorcycle to motor vehicular incident ratio of 1:1.2, this went contrary to our expectation. We had expected the reverse as was the finding in our recent study on head injury, and the reason for this situation is not very clear to us, though it appears that in our previous study more head injuries than spinal injuries occurred with motorcycle passengers, none of whose victims wore protective helmets22 . Sport and recreational injuries were very small in our series unlike what is obtained in published reports, further buttressing the fact that we lack the facilities for these healthy activities in our trading sub-urban community1,2,3,4 . Noteworthy and worrisome is the fact that we evaluated most of our cases 58(93.5%), with plain radiography alone and only a paltry 3(3.48%) with computerized tomography. It is widely accepted that evaluation of cord injuries is best done with magnetic resonance imaging which is known to give better details on the extent of neural injury, as well as predict possible neurological outcome10,18. Our centre does not have facilities for MRI, and even for the few that did CT scanning, these were done in another centre where the facility was available and the indication in all 3 cases was our inability to arrive at a definitive diagnosis of the vertebral lesions based solely on plain radiography. With the inadequacy of this imaging modality, there is no doubt that we would have missed some important soft tissue lesions, a situation which could have impacted significantly on our outcome, not least the mortality. Complete cord injuries represented more than half of our cases contradicting the findings of Stover and Young, et al, in whose different series incomplete injuries superceded9,11,12 . This disparity could be explained by the fact that whereas we used the Frankel scale to evaluate completeness of injury, these other workers made their assessment based on the ASIA scale. All our cases were treated non-operatively, using Gardner-Wells’ tongs traction for cervical injuries and postural reduction for thoracic and lumbosacral injuries, simply because beyond the bony lesions imaging modality could not ascertain the presence or otherwise of other surgical lesions. Our outcome from complete and incomplete injuries, nonetheless, were consistent with several other previous findings, where all cases of complete injury made no neurological gains, while cases of incomplete injury recovered functions to various extents19,20,21. Whether this situation would persist remains to be seen since the longest duration of follow-up was 11months and only 19(30.6%) cases were followed up for a mean duration of 3months; and the rest did not turn up after discharge. Mortality was 13(21%), which is comparable to the findings by other workers23 . Remarkably, all the cases of mortality had cervical cord injuries. Conclusion Spinal injury, which was consistent with the universally reported patterns of distribution in most of our parameters, was an important indication for neurosurgical consultations in our service, but optimal care was severely hampered by the lack of modern imaging facilities. Complete cord injuries were more in number than incomplete injuries contrary to other previous reports, and the case incidence from motorcycles was remarkably high. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09013t1.jpg] [js09013t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}