 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
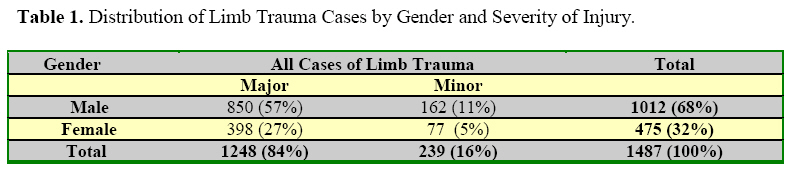
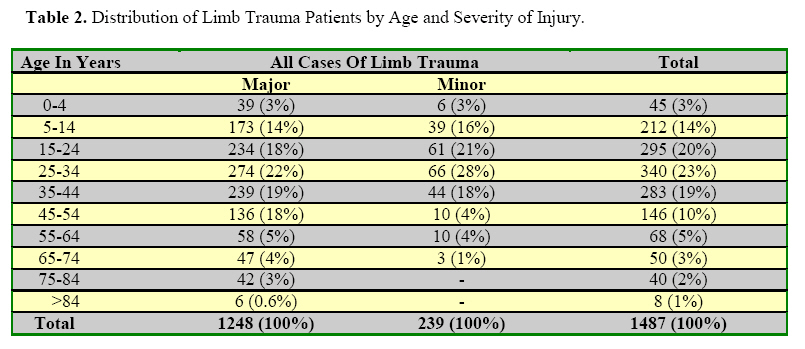
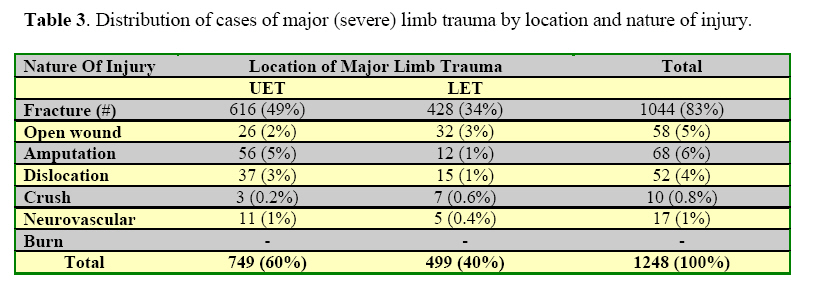
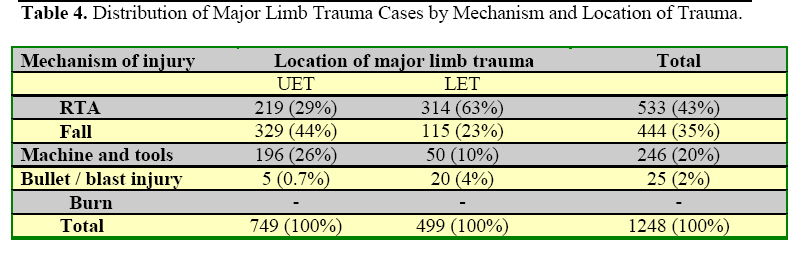
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 84-87 Major Limb Trauma in Eastern Ethiopia. Munyazewal Dessie, MD Department of Orthopaedic Surgery, Dilchora Hospital, Dire Dawa, Eastern Ethiopia. E-mail d_manyazewal@yahoo.com. Code Number: js09015 Background: Disability following road traffic accident is expected to increase dramatically in developing countries resulting in a decline in the size of the labour force. Adolescents and young adults are at the greatest risk of limb injury resulting from road traffic accidents. The objective of the study was to identify patterns of major limb trauma based on the definition given by the WHO scientific group. Introduction Road traffic accidents are among the top ten causes of mortality and the disease burden. Disability following road traffic accident is expected to increase dramatically in developing countries resulting in a decline in the size of the labour force. Adolescents and young adults are at the greatest risk of limb injury resulting from road traffic accidents1,3 . The global health burden of injuries in the year 2020 is protected to be equal to that of communicable diseases, and to be even greater in some developing countries. Injury related problems are expected to be higher in Ethiopia sue to recent increase in industrialization, road traffic and the use of unsafe technology and working conditions 2,3,4 . Out of all musculoskeletal injuries nearly 50% are to the upper limb and 36% of injuries to the lower limb (RR = 1.4)3. Of all injuries upper limb fracture accounts for 12% and lower limb fractures for 10% (RR = 1.2). RTA’s, fall, machine and tool injuries in this decreasing order of frequency are the leading causes of limb injuries3,4,5 . Trauma caused 222% of major upper limb amputations and 18% of major lower limb amputations (RR = 1.2). RTA’s, fall, machine and tools were respectively the caused of 45%, 11% and 9% of major limb amputations6. Operational definition: The definition of major (severe) limb trauma according to a WHO scientific group includes all fractures, dislocation, crush injuries, open wounds, amputations, burns and neurovascular injuries to the extremities1. Spine, mandibular, nasal and skull fractures are not included in the definition and are hence excluded from my audit. The objective of the study was to identify patterns of major limb trauma based on the definition given by the WHO scientific group. Patients and Methods Dilchora Hospital is the only government health facility providing specialised orthopaedic and trauma management in the Eastern part of Ethiopia which has a population (catchment area) of about 5 million. The hospital has 230 beds, of which 24 are for orthopaedic and trauma patients. There is only one specialist orthopaedic surgeon available, but general surgeons and general practitioners provide some orthopaedic and trauma care. This audit was conducted by the author who recorded the relevant findings on every patient that was referred to the orthopaedic department between October 1st 2004 and April 31st 2007. Results During the two and half years 1487 (1012 males 68%, 475 females 32%) were managed by the author. This is a sex ratio of 2 to 1. Of this grand total, 1248 (84%) were considered to have suffered major limb trauma (Table 1) and 883 (70%) were between the ages of 15 and 54 years (Table 2). The upper limb was injured in 749 (60%) and the lower limb was injured in 499 (40%). The categories of injuries are summarised in Table 3, and to note there were no burn injuries. The responsible agents of injuries are shown in Table 4 and as seen RTA’s were the leading cause. Discussion The results of this audit showed that the majority (70%) of major limb trauma occurred in the 15 and 54 years age group. People of working age are largely affected by major limb trauma and this finding is similar to that reported by a WHO scientific group and by others authors1,3,4 . Major limb trauma occurred more in the upper limb than the lower limb (RR =1.5). This is consistent with other reports3,5,6. Fracture, dislocations and traumatic amputations accounted for the majority (93%) of the diagnosis in the identified patterns of major limb injuries. Previous study at TAUH agrees with the finding4. RTA, fall accidents, machine and tools in their order of decreasing frequency are the leading causes of major limb trauma in the Eastern part of Ethiopia. Many reports showed similar results1,3,4,5,6. These are preventable causes seriously affecting the labour forces in our country. Improving roads (design, construction, complete separation of pedestrians from vehicles), traffic education of drivers and the public in general, establishment and enforcement of health and safety measures at work (e.g machine guards, protective gear) are suggested to be implemented to reduce the size o f the problem. Conclusion and Recommendations To reduce the economic impacts of major limb trauma I suggest:
Acknowledgement I would like to express my thanks to Professor Goefrey Walker FRCS for his help in the preparation of this manuscript. The cooperation of Dr. Tezera Chaka, Head -Department of Orthopaedic Surgery, AAU, is appreciated. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09015t4.jpg] [js09015t1.jpg] [js09015t2.jpg] [js09015t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}