 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
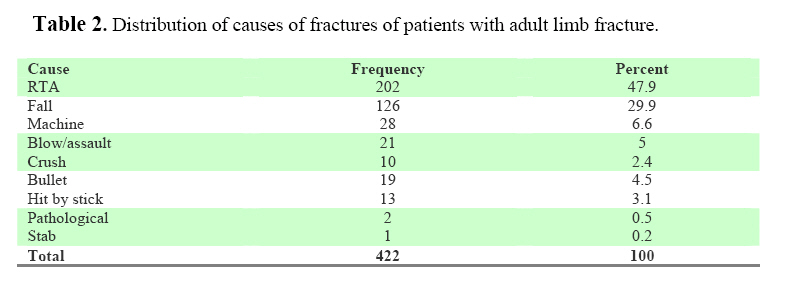
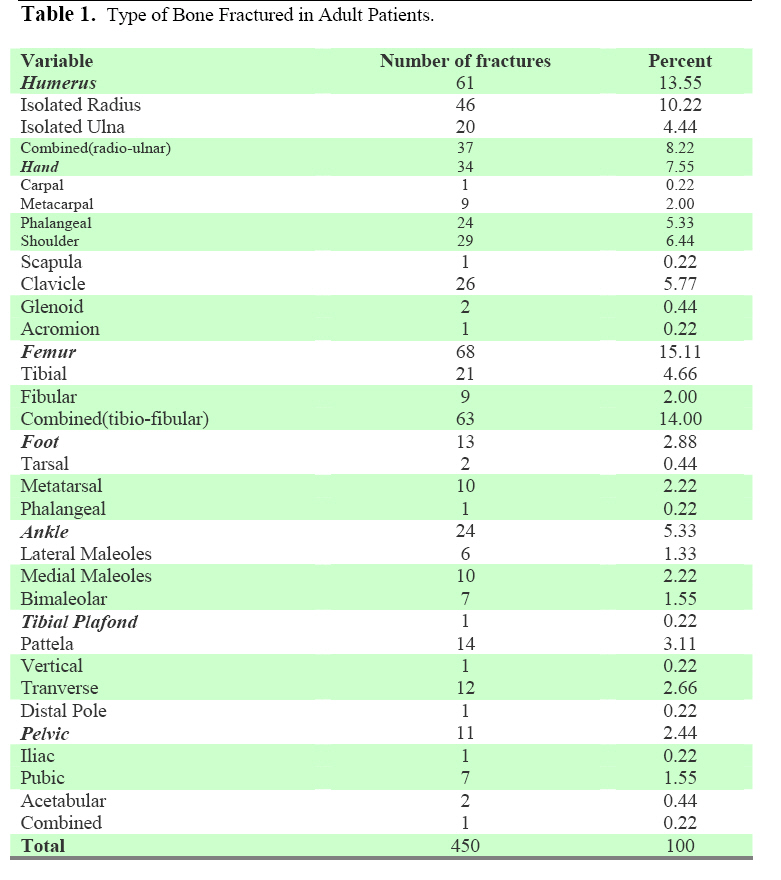
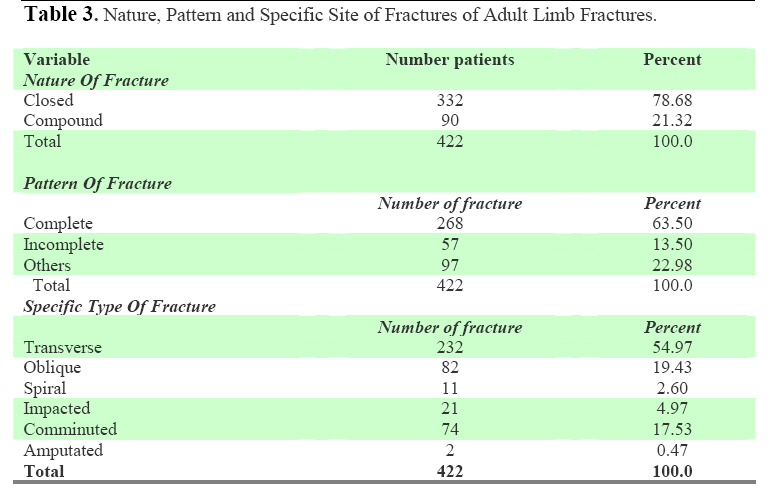
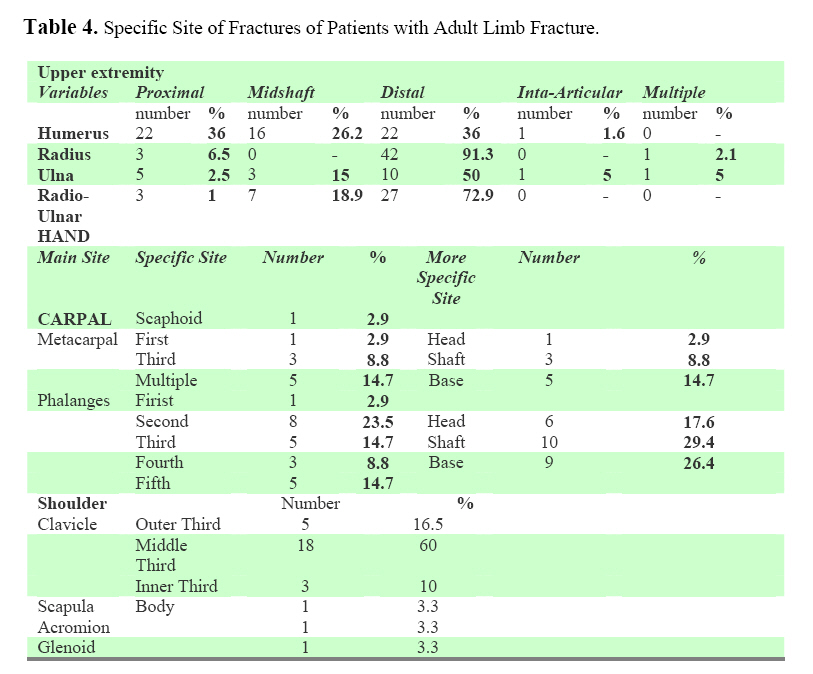
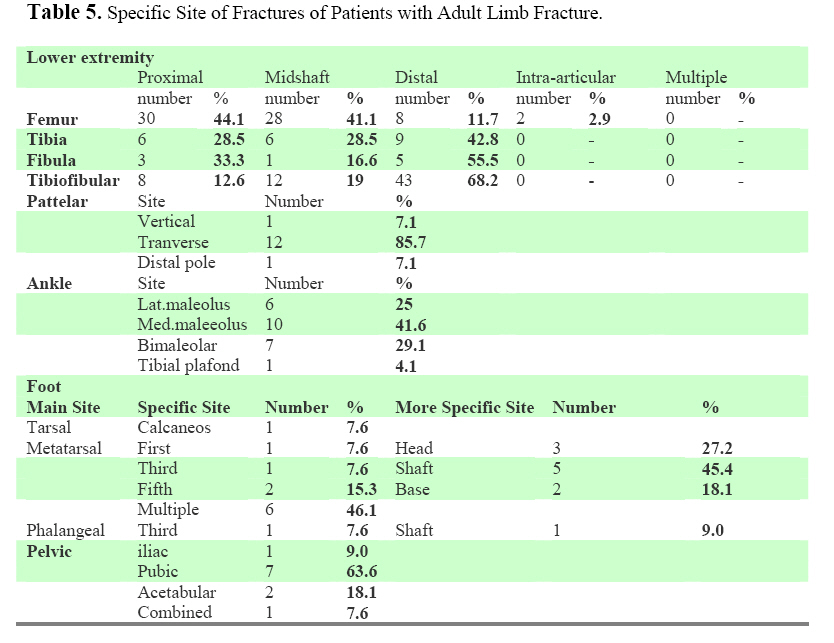
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 88-97 Radiological and Clinical Details of Major Adult Limb Fractures in a Teaching Hospital, AAU, Ethiopia. D. Admasie1, Y. Tekle Y2, B.L. Wamisho3 1Associate. Professor of Radiology, Addis Ababa University, Medical Faculty (AAU-MF) Code Number: js09016 Background: This prospective study done at Addis Ababa University, Medical Faculty, Department of Radiology, Tikur Anbessa Hospital was aimed at determining the causes, magnitude, radiological and Clinical patterns of major limb fractures in adults in a half-year period from March to August 2007.In Addis Ababa University, fractures are managed both conservatively and operatively, but for lack of implants or expertise, patient which should have been treated surgically are managed conservatively and stay very long (average hospital stay of 11 days) in the Hospital. Such knowledge helps to plan on the management of the fractures and resource-recruitment. . Introduction Ethiopia is a country located on the Eastern part of Africa. It is a predominantly Christian (63%) developing country with a population of 74 million and a current annual population growth rate of 1.3% where little attention is given to injuries (1, 2). Injuries constitute around a half of all surgical emergencies (3) and were the primary reason for an emergencies hospital visit in Addis Ababa during 1999(4). Road traffic crushes are the commonest cause of injury in urban area in Ethiopia with 199 fatalities per 10,000 licensed vehicles per year (5,6). Thus identification of the condition as one priority area coupled with effective and efficient resource allocation, health policy and management would make a difference in the diagnostic and therapeutic perspective of major limb trauma and orthopedic emergencies. Fractures may occur under a variety of clinical circumstances. Most commonly, a fracture is the result of a large force acting acutely on an otherwise normal bone, and disrupting the normal bony architecture. According to the 1996 world Health organization report (WHO) injury ranks fifth among all causes of death and accounting for 5.2% of all mortality worlds wide (7). It is a leading cause of death and disability for people under 45 years in the industrialized world (8,9). These rates are declining in developed countries but injuries are important and a largely neglected health problem in developing countries (9). Fractures involving the long bones in adults should be described using certain universally accepted descriptive conventions (10). Transverse fractures are those that run at right angles orthogonal to the long axis of the affected bone. Oblique fractures, cross the shaft at an angle. If the inciting injury involved significant torsion, a spiral fracture may occur; the fragments created by a spiral fracture are often very sharp and pointed, and may cause significant soft tissue injury. Any fracture that divides the bone into more than two separate fragments is said to be comminuted; the degree of comminution is often directly related to the force of the injury. Although it may seem obvious, the location of the fracture should be described in precise terms. In general, the location of fractures involving the shaft of a long bone can be described by dividing the shaft into thirds (proximal, middle, and distal), and placing the injury by reference to this division (e.g. 'junction of the proximal and middle third of the shaft', 'mid-shaft').The type of fracture is important. Clinically, perhaps the most important feature of a fracture dictating its management is the distinction between open fractures (in which the overlying skin is disrupted and the fracture is connected with the outside environment) and closed fractures (in which the overlying skin is intact). This distinction is usually best made on clinical grounds, although subtle radiological clues, such as gas in the adjacent soft tissues, may suggest previous transient exposure of the bone to air in the absence of obvious clinical evidence. Fractures extending right across a bone (i.e. involving 'both cortices' radio graphically) are called complete fractures. Similarly, fractures that do not extend all the way across the bone are referred to as incomplete. Our study at “Tikur –Anbesa” university Hospital is aimed at determining the volume and categories of major limb trauma requiring emergency treatment and the relative incidence of specific fractures. A prospective study of the incidence of fracture in the adult population of Edinburgh, related to age and gender. Over a two-years period ,15293 adults,7428 males and 7865 females, sustained a fracture .There was a higher incidence of fractures in men than women in all age groups from 15 to 49 years. The total male incidence is bimodal, with peaks at 20 to 24 years and 90 to 94 years. Females had a smaller peak from 20 to 24 years, with a steady increase later from 46 at 40 to 44 years to 774 per 10 000 population per annum in females aged 90 to 94 years. Under the age of 35 years males are 2.9 times more likely to sustain a fracture than females .Over the age of 60 years females are 2.3 times more likely to sustain a fracture. As regards hip fractures there was no significant gender difference from 15 to 60 years, with zero to five cases per 10 000 population per annum. Over 60 years the incidence rose in both genders and the common odds ratio from 60 to 94 years was 1.9 more for females (11).Pelvic fractures showed a similar pattern with an overall incidence of 0 and 3 cases per 10 000 population per annum from 15 to 59 years. After this age the female incidence rose from 3 to 67 cases per 10 000 population per annum, and the male incidence from 1 to 17 cases. The incidence of wrist fractures in under 40 years was 1.4 times more likely in males. But after this there is an almost linear rise for females of about 10 cases per 10 000 population per five-year group. With regard of incidence of diaphyseal fractures, in fractures of the humeral shaft there was no obvious gender difference, with relatively constant rates between 15 and 64 years at about 0 and 2 per 10 000 per annum. After 65 years the rate rose. The incidence of forearm fracture was generally low (at 0 to 4 per 10 000 population per annum), but consistently higher for males from 15 to 44 years. The incidences of femoral and tibial shaft fractures in both the rates are greatest in both the young (15 to 34 years) and the elderly (over70) age groups. There are minor gender differences in the rates of elbow or knee fractures, but ankle fractures are more common in young men. In the elderly, both ankle and proximal humeral fractures are more common in women. Shaft fractures were more common than end (metaphyseal) fractures only in the femur in young adults. End fractures were more common than shaft fractures in the forearm and tibia in all age groups, and in the humerus and femur after the age of 35 years. A study on epidemiology of humeral shaft fractures was done at the Royal infirmary of Edinburgh, Scotland (12). They have analyzed 249 consecutive fractures of the humeral shaft treated over a three-year period. The fractures were defined by their AO (Association for Osteosyntesis) morphology, position, the age and gender of the patient and the mechanism of injury. Analysis showed a bimodal distribution of the fractures. The peaks were in the third and seventh decades with the division at 50 years of age .In the under 50-year group, 70% of the fractures occurred in men and over twothirds were the result of moderate to sever trauma. Over 60% of fractures occurred in middle segment of the shaft of the humerus .In general an increasing severity of fractures as defined by the AO type were seen consequent to more violent injury ,with 40% of fractures sustained by pedestrians in RTAs being AO type C.Less than 10% of the fractures were open.A study on epidemiology of tibial fractures was done at the Royal Infirmary of Edinburgh, Scotland (13). They performed an epidemiological analysis of 523 fractures treated in the Edinburgh orthopedic Trauma Unit over a three-year period .The average age of the patients were 37.2 years (12 to 98).There were 400 closed fractures (76.5%).The average age of these patients was 35.6 years. There was an increase in severity of the fractures with age.123 were open fractures 59.8%.Fractures of the middle and distal thirds were relatively common. Road-traffic .accidents (37.5%) and sport (30.9%) accounted for most tibial diaphyseal fractures with simple falls causing most fractures in the elderly. The fibula was intact in 117(22.3%) of the tibial diaphyseal fractures. The average of the patients in this group was 30.4 years. Other study was done on fracture of the clavicle in the adult at the Royal Infirmary of Edinburgh, Scotland (14). From 1988 to 1994 medical records and radiographs of 1000 consecutive adult patients with fracture of clavicle was analyzed. It has been estimated that fractures of the clavicle account for 1 in 20 of all fractures and 44% of all injuries to the shoulder girdle. The incidence of all fractures in adults over the age of 13 years remained constant over six years at 29.14 fractures per 100 000 population per year. Fractures were most common in males under the age of 30 years typically as a result of a contact sport or after an RTA .fractures in females were more constant with age ,with a smaller peak in those under 30 years age. The usual mechanism of the fracture, irrespective of site, was a direct force applied to the point of the shoulder such as occurs during a fall or RTA. Finally, knowing the magnitude, nature, pattern and site of fractures commonly presenting to an institution helps in planning on their treatment ( Surgical Vs conservative) and it also helps in developing an efficient system in terms of directing resources( implants, operating time physiotherapy)(15) . Methods This study was a cross-sectional, institution based prospective study with both radiological and orthopedic variables were reliably assessed. The study included all the major limb trauma patients who attended the 'surgical' and orthopedic Emergency department of “Black-Lion Hospital”, B.L.H and had fracture at the same time. A single population and a single population proportion formula, n = (Z α/2)2 p (1-p) / d2, was used to estimate the sample size. Since the investigator didn't get such a study showing the proportion of patients among those patients presenting with major limb trauma and attended the 'surgical' Emergency department of T.A.U.H to achieve a conservative sample size sufficient enough to make a valid statistical computation and conclusion, the following assumption was made: proportion of patients with fracture as 50% (p = 0.5), level of significance to be 5% (α = 0.05), and absolute precision or margin of error to be 5% (d = 0.05). Computing with the above formula gives a total sample size of 384. Considering a 10% non-response rate would finally make the sample size 422. Data collection related to radiological variables were done by the research team to help reduce inter-observer measurement variability. “Difficult” patterns were discussed further. All radiographs were read by the radiologist Those research subjects with insufficient data with regard to important variables and data related to research question and objective were excluded. Operational definitions: Adults were aged 12 years or over. Statistical Analysis: The data were entered; cleaned and analyzed using Epi Info-2002 version 6 and MS-Excel 2007.Appropriate significance tests and trend equations were also done. Results A total of 422 adult patients aged between 13 – 90 years (mean = 34.96, median = 39.5, and SD. = 15.8) who attended the surgical and orthopedic outpatient emergency department of “Tikur Anbesa” University Hospital with major trauma were studied for fracture of long or short bones over six months period from March to August, 2007. Most of the study subjects, 318(75.4%) were males and the rest, 104(24.6%) were females making male to female ratio of nearly 3:1. The highest age group mostly affected was between 21-30y (36.5%) and the highest peak of male to female ratio occurred in the age group between 31 to 40 years which was 5.2: 1. In all age groups the proportion of males is higher for males than for females. The majority of the subjects 344(81.5%) were urban residents whereas only 78(18.5%) were from rural settings. Eighty nine (21.5%) were daily laborers, 65(15.4%) house wives, 53(12.6%) farmers, 53(12.6%) students, 46(10.9%) office workers, 22(5.2%) merchants 22 (drivers) and others 72(17%) by occupation . The proportion of daily laborers, house wives and farmers and students constitute the first three ranks respectively with the proportion of males in daily laborers, farmers and students being higher than females (P < 0.05). Several causes responsible as to the etiology of fracture from traumatic to none traumatic factors were identified and nearly all the fractures 420(99.5) were due to traumatic incidents but only 2 (0.5%) were due to pathological fracture (Table-2).Road traffic accident constitutes the largest proportion, 202(47.9%), among traumatic causes followed by fall down accident 126(29.9 %) and blow assaults 28(6.6%) (Table-2) With regard to bone involvement, the highest frequency of fractures occurred in the femur 68(15.1%) followed by tibio-fibular 63(14%) and humerus 61(13.5%) (Table-1). It was evident that upper limbs or lower limbs were included solely or simultaneously. Injuries to the upper limb alone accounted for 50.53% whereas the proportion of injury for the lower limbs was 49.42%. It was also recognized that the fracture was either single or multiple at different sites. The proportions of fractures at a single site or multiple sites were 99.55% and 0.44% respectively (P<0.05). Among the single site fractures, 227(50.4%) were in the upper limbs and 223(49.55%) in the lower limbs. However the multiple sites fractures were 0.44% and 0% for upper and lower limbs respectively . Different variants in the nature, pattern and type of fracture were observed.The nature of the majority of fractures noticed were closed fractures accounting 332(78.68%),compound fractures were smaller in number and proportions only responsible for 90(21.3%) (Table 3). The pattern of the majority of the fractures that occurred was complete in 268(63.5). Incomplete fractures comparatively accounted smaller proportions 57(13.5%), others were 97(22.9% (Table 3). With respect to the pattern of fractures, transverse fractures stands out the first 232(54.9%) fallowed by oblique 82(19.4%) and comminuted 74(17.5%) at the 2nd and 3rd place respectively among the different specific type of fracture. Spiral fractures were 11(2.6%) and amputated fracture, 2(0.5%), accounted for the least proportion of patterns of fractures .Finally side of fractures were analyzed and the right side was slightly more involved accounting 236(52.1%) as compared to the left side 211(47.2%) and 3(0.6) had involvement of both sides. This study revealed that the proximal and distal fractures for humerus occurred with similar proportion, 22(36.1%) for each while mid shaft fracture accounted for 16(26%) of fracture of the humerus. For radio-ulnar fractures the distal third fracture, 27(73%), accounted for the majority of fractures. The distal fractures accounted for the largest proportion, 42 (91.3%) of fractures of the radius as compared with the proximal, 3(6.5%) and multiple, 1(2.2%) fractures (Table 4). Femoral fractures were higher in proximal third 30(44.1%)fallowed by middle third 28(41.1%) and distal third 8(11.7%).Tibial fractures were higher in the distal third 9(42.8%) fallowed by middle and distal third each 6(28.5%). Fibular fractures were higher in the distal third 5 (55.5%) fallowed by proximal third 3(33.6%) and middle third 1(16.6%).Tibio-fibular fractures were higher in the distal third 43(68.2%) fallowed by middle third12(19%) and proximal third 8(12.6%) The distribution of fractures with regard to the specific sites of the bones is illustrated in (Table 5). Discussion This study revealed that out of the 422 study participants, the majority of people who sustained injury and presented with fracture were residing in urban (Chi-square = 167.7, P < 0.001). This is mainly due to the fact that this study was done in Addis Ababa and the majority of trauma cases who will come to Tikur Anbesa Hospital are residing in the main city. With regard to age and gender, (83.4%) of the trauma cases occurred in the age group below fifty years with the male to female ratio of 3.6 (P <0.05).The highest age group mostly affected was between 2130y(36.5%) and the highest peak of male to female ratio occurred in the age group between 31 to 40 years which was 5.2: 1.This finding was similar to other reports from our Hospital. In all age groups the proportion is higher for males than for females. This was also a consistent finding with the prospective study of incidence of fractures in the adult population of Edinburgh in January 1999. Under 35 years of age, males were 2.9 times more likely to sustain fractures than females (95% CI 2.7 to 3.1.). The study done on orthopedic and major limb Trauma at the Tikur Anbessa University Hospital, Addis Ababa, Ethiopia between December 2001 and November 2004 showed that males were more affected (73.3%) than female (26.1%) giving a male to female ratio 3:1 and this is also consistent with our study. The study also revealed that fractures are more common in daily laborers, house wives, farmers and students (P<0.05). With regard to the cause of injury, road traffic accident accounted for the majority of the traumatic causes of fracture 47.9%), (P-value< 0.0001). Males were affected more commonly than females with male to female ratio 2.8-1 which also showed similar result to other comparable studies which showed male to female ratio 3:1. The top three causes of fracture 9 Table 2) remained the same and this was noted by the two decade analysis for trends of disability following injury (16) .Other causes of injury also showed higher male affection than females which was statistically significant finding except for stick injury and pathological fracture where the total number of the cases is insufficient for statistical analysis. There was only one case of stab injury who was a female. This was also a consistence finding with the study done in Kampala between 25 September and 11 December, 1997, where 35.1 % of all the trauma cases were due to road traffic accident with a high male to female ratio (17). Similar study done at Nigeria teaching hospital showed that among 349 patients with injury 137 patients sustained R.T.A which accounted 38.8% of all injuries with high male to female ratio(18).A study done by Mulat and et al at T.A.H also showed among the 3822 injured patients in the study 40% were R.T.A(4). This was also a consistent finding with our study. Fall down accident was the second commonest cause of injury accounting 29.9% of the total trauma in our study and this was slightly higher to that studied in Nigeria which accounted 21.4% and also was the second commonest cause of injury and slightly lower to similar studies and this could be due to our relatively small sample size. A study done on patterns of childhood fractures in Khartoum disclosed that none road-accidents accounted for 84% of the fractures mainly due to sports, domestic injuries and falls; whereas road traffic accidents were 16% and occurred mainly in pedestrians. The long bones were affected in 91% of all fractures, the commonest site being the distal end of forearm 26%, fallowed by supracondylar fracture of the humerus 15%. In the upper limb, left sided fractures predominated. Open fractures constituted 9.8% of the series (19, 20). This showed that that the commonest cause of injury and site of injury in adult and children is quiet different (20) . Considering the site of injury, fracture of the femur, tibio-fibular and humerus accounted for the majority of the cases (X2=212.1, P< 0.001).Injuries to the upper limb alone accounted 50.4%.whereas the proportion of injury for the lower limbs was 49.55% . A study done by Elias and et al between December 2001 and November 2004(21) showed that upper and lower limbs were injured in almost equal proportions, 49.7% and 43.5% respectively. Analysis of the nature of the fracture revealed that closed fracture were significantly more common than compound fracture (chi-square= 138.8, P < 0.01). Considering the pattern of fractures as complete or incomplete, there was a statistically significant different finding. Two hundred sixty eight were complete whereas only 57 fractures were incomplete (X2=136.99, P < 0.01). Although not statistically significant, analysis of the distribution of fractures with regard to bone involvement revealed that fracture is common on the right side for radio-ulnar, ulna, Hand, femur, tibio-fibular, Ankle and Foot-(P>0.05). Fracture is more common on the left side for humerus, radius, Shoulder, tibia, fibula and Patellar fractures (P>0.05).The proportion of fractures was similar on both sides for pelvic fractures. A study done on the epidemiology of humeral shaft in Edinburgh, Scotland (11) revealed that most fractures (60%) occurred in the middle third of the diaphysis. This study revealed a different finding. Only 26.2% of humeral fractures occurred in mid-shaft and fractures of the humerus occurred with the same proportion in the proximal and distal humerus which was 36.1% for each (P> 0.05). Based on the study the following are our recommendations:
Acknowledgment We thank the patients for co-operating in the study. We thank the department of Radiology and Orthopedics in the Medical faculty. Special thanks to Dr Belete Zergaw and Dr. Mohamed Abseno (MD, MPH) for their great help and advice in the analysis and discussion of results. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09016t5.jpg] [js09016t4.jpg] [js09016t1.jpg] [js09016t2.jpg] [js09016t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}