 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
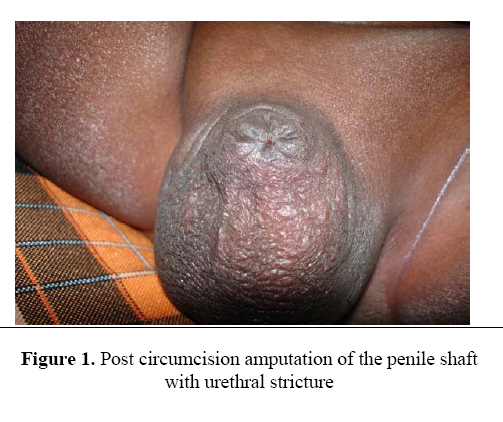
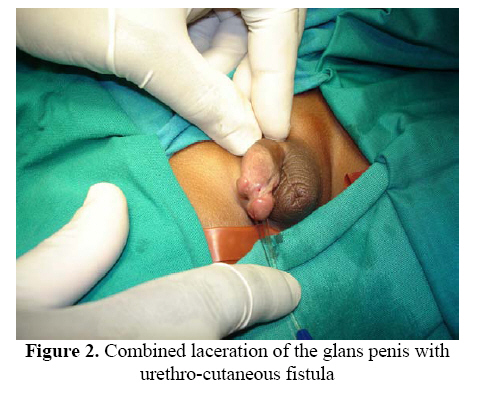
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 109-113 Circumcision Mishaps: A Continuing Challenge In The Developing Countries O.A. Sowande, O. Adejuyigbe Paediatric Surgery Unit, Department of Surgery, Obafemi Awolowo University Teaching Hospital, Osun State, Nigeria. Code Number: js09019 Objective: Circumcision has been described as the most commonly performed surgical operation in the boys and is probably the oldest surgical procedure in man. This prospective study was aimed at establishing the pattern, treatment outcome and cost of major complications of neonatal circumcision seen in a tertiary center in Nigeria. Introduction Circumcision is probably the commonest surgical operation done in childhood with an estimated one-sixth to one-quarter of the world male population circumcised1,2. Neonatal circumcision is practiced worldwide and is suppose to be easier and less associated with complications3. While there are debates as to the appropriateness of circumcision in boys, there is some evidence that circumcision reduces the incidence of urinary tract infections in young boys and may be protective against Ca penis and cervical carcinoma4-8 . As frequently as it is performed, the procedure is not devoid of complications. The incidence of complications following circumcision has been estimated to be approximately 0.2% to 0.6% in the United States but could be as high as 55 per cent9,10. The majority of complications were minor, the most common being local infection and bleeding. In Nigeria circumcision is routinely performed for non medical reason and the prevalence of male circumcision is high with more than 80% of the males are circumcised11,12. The rate of post circumcision complication is however unknown. Our observation over the years suggests that circumcision is less frequently done in our hospital compared to few years back but the rate of referred complication is on the increase. This prospective work is to document the pattern, treatment outcome and cost of major complications of neonatal circumcision seen in a tertiary center in Nigeria. Patients and Methods All patients presenting to the Paediatric surgical unit of the Obafemi Awolowo University Teaching Hospital Ile Ife, Nigeria with complications of circumcision were prospectively studied over a period of 3 and half years from July 2003 to December 2006. Information regarding the age of the patient, time of circumcision, the surgeon, place of circumcision was recorded as well as the type of mishap and outcome of management were noted. During the same period data on the number of circumcision done in our hospital and any associated complications in was collected Results During the study period, there were 728 new patients referred to the outpatient surgery unit of the hospital. Of these there were 45 patients with major complications of circumcision representing 6.2% of the patient load. Their age at presentation ranged between 2 weeks to 10 years (Median = 3months). All the patients were circumcised during the neonatal period. During the same period, 104 circumcisions were done in the unit using the bone cutter method and Plastibel. There were no complications observed. Types of complications The commonest complication reported is urethro-cutaneous fistula in 25 (56%), Meatal Stenosis in 4(8.9%), Severe bleeding in 4(8.9%), Epidermoid cyst in 3 (6.7%), and 2 (4.4%) cases each of Buried penis, penile amputation, penile degloving with glans amputation, glanular adhesions and redundant prepuce respectively. The fistulae were located at the corona or just beyond the corona on the ventral surface. No dorsal fistula was seen. In two patients it was located on the lateral side. The circumcision was done by nurses-mostly community health officers in 28 (62.2%), traditional surgeons in 10 (22.2%) quacks in 4(8.9%), and medical doctor in 3 cases (6.7%). Treatment and Outcome Patients with urethra-cutaneous fistulae were treated with layered closure using 5/0 or 6/0 polyglactin sutures. Four (16%) patients had Mathieu like flap repair. All the patients had suprapubic or urinary catheter diversion of urine and were hospitalized for a period of 7 to 12 days (Figure 1). Two required re operation because of failed repair. Bleeding was controlled with sutures in all the four patients with bleeding with only one of them requiring blood transfusion. All the meatal stenosis had meatoplasty as day cases with satisfactory result. The epidermoid cysts were excised under general anaesthesia as day cases. Patients with redundant prepuce had re-circumcision using the open dissection method. The patients with penile degloving also had glans amputation but presented late hence were managed conservatively with wound dressing and the final outcome was acceptable to the parents. The buried penises were managed with mobilization of local skin flaps for penile coverage after de-gloving the penis. The two patients with penile amputation also presented late. One of these patients had associated urethra stricture and urinary retention. The stricture was dilated and urethral catheterization done. The two are still awaiting definitive surgery. The cost of treatment for the repairs varies from 4500 -35,000NGN (40-305 Dollars) Discussion Circumcision has been described as the most commonly performed surgical operation in the boys and is probably the oldest surgical procedure in man. There are various techniques of performing circumcision, the aim of which is to provide the best cosmetic result together with the lowest possible complications. In any technique, asepsis, adequate excision of the inner and outer preputial layers, haemostasis and cosmesis is important13. There are rare reports on the pattern and magnitude of circumcision complication in our environment. A hospital survey of infants attending a child welfare clinic in South Western Nigeria found an incidence of 20.1% complications of circumcision in 370 boys11. This suggests that most complications following circumcision are minor and many are not reported in the hospital. However, major complications such as severe bleeding, fistulae and glans amputation may occur, and require surgical intervention. These are bound to be reported to the hospital because of their magnitude and parental anxiety. This study showed however that presentation may be delayed especially urethro-cutaneous fistulae which may not interfere with the child’s ability to micturate and because of financial constraints Most of the complications after circumcision in our series were due to mechanical faults caused by the poor surgical technique of inexperienced personnel. It should be noted that nurses, doctors and the laymen practicing circumcision in our community do not undergo any formal training in the art of circumcision. Circumcisions are more frequently performed by clamping and guillotine-like incisions. Application of this technique by inexperienced personnel who have learned the technique only by observation can lead to glandular, urethral and corporal injuries2. Urethro-cutaneous fistula following circumcision may occur for a variety of reasons but, the reported incidence of this complication is low2. However in this series it constituted the commonest complications referred to our clinic for correction. The proposed the commonest cause is a poorly placed suture at the frenulum in an attempt to obtain haemostasis14,15. However the most commonly employed technique by the surgeons in our environment is the guillotine technique and no suture materials are applied in most cases. It is postulated that excessive traction on the ventral penile skin pulls part of the urethra into the incision hence direct trauma is the most likely cause. In most individuals the fistula only became obvious at the 3rd to 5th day following separation of the dressing. In the majority of our patients the fistulas were located on the ventral surface very near the corona. In two patients the fistulae were located on the lateral side of the corona. The sepsis and penile or urethral anomalies have also been implicated in the aetiogenesis of these fistulae is16,17 but this is difficult to determine in our patients. Although there are many approaches to the management of such a urethral fistula18,19 we have applied layered closure in most instances with good success. We have had to use local penile flaps (Mathieu) in four patients. All the patients had urinary diversion with suprapubic cystostomy or urinary catheter drainage postoperatively. In cases of corporal amputation where the child is older and the incision is suit-able, such incisions are reported to be treated by successful anastomosis in clinics with highly improved facilities2,20. The two patients in this series had their penile shaft completely cut off and did not present early although facility for reattaching the phallus with microsurgical techniques are not available. Also there is currently a dilemma as to the appropriate treatment in our environment as female sex conversion is generally unacceptable to our patients. This current study was stimulated because of the observation that the rate of circumcision in our hospital has been on the decline over the last few years and the apparent increase in the number of patients presenting with complications of circumcision. The study showed that most complications occurred in local maternity and health centers and private hospitals and majority were carried out by nurses. Apart from the morbidity associated with these complications, there was a significant increase in the cost of repair. Most of the parents are poor and the reason why the circumcision was done outside the hospital was because of cost. Unfortunately most of them had to spend multiple amounts for the treatment of these complications. The authors believe that the issue of circumcision should not be trivialized. The load of circumcision however can not be borne by medical doctors in secondary and tertiary centers alone. We strongly believe that educating society about this matter is important. We are not aware of any legislation regarding circumcision in our country. Primary circumcision performed by laymen carry a high complication rate and serious complications may occur (21-23). It is suggested that laymen and traditional surgeons who wants to perform circumcision should undergo a period of training and direct supervision by physicians is done before allowing laymen to perform circumcision independently. The authors’ also belief that training workshops for nurses and doctors would go a long way in reducing the incidence of these complications References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09019f2.jpg] [js09019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}