 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
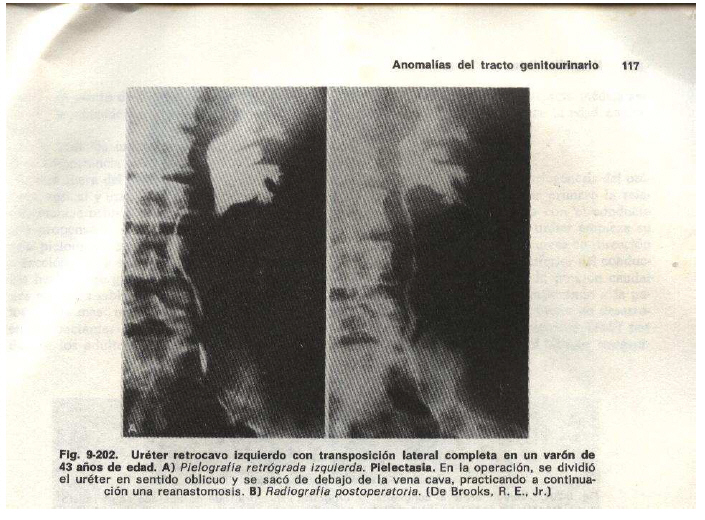
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 119-121 Retrocaval Ureter with Ureterohydronephrosis A.Tegegne, C. Cobas Urologic Surgeons Code Number: js09021 Retrocaval ureter is one of the rarest congenital anomaly. We report a case of retrocaval ureter who presented to us with right lumbar pain, with ureterohydronephrosis. The intravenous urography showed dilated proximal ureteric segment with moderate hydronephrosis. The patient was operated, findings were Retrocaval ureter and a ureteroureterostomy with anteriorisation of ureter was performed. Introduction Retrocaval ureter is one of the rarest congenital anomaly. It is a condition in which the ureter deviates medially and passes behind the inferior vena cava, winding about and crossing in front of it from medial to lateral side. It was first reported by Hochstetter in 1893.2 Incidence of retrocaval ureter is one in 1500 cadavers.1,3 Male to female ratio is 3 or 4:1. Most patients present with right lumbar pain. They may have recurrent urinary tract infection or episodes of acute pyelonephritis. Occasionally calculi may form above the obstruction and symptoms may be attributed to these. Case Report A 22 years old male presented with right flank pain aggravated by supine position since the past one year. The pain was of sudden onset, intermittent and colicky. He had also occasional left flank pain, frequency and urgency of urine. Had low-grade intermittent fever. Initially he has hematuria. On general examination, no abnormality was detected. On per abdomen examination, the patient had pain in the right lumbar region, right flank and right renal angle. He had no rebound tenderness. The per rectal examination was normal. A complete laboratory evaluation was done. His haematological profile was within normal limits; the serum electrolytes were normal and so were his blood urea nitrogen and creatinine values. Urinalysis was normal. Ultrasonography of the abdomen revealed right side chronic obstructive uropathy secondary to retrocaval ureter. Intravenous urography showed hydronephrosis with proximal hydroureter on the right side. The left kidney, left ureter and urinary bladder were normal. The right kidney and ureter were approached by right subcostal incision below the twelfth rib. On exploration, right proximal ureter and pelvis were moderately dilated. Dilated proximal ureter curved medially, then posterior to the inferior vena cava, finally curved anteromedial to the inferior vena cava and took a downward course. The distal ureter was normal. Procedure Ureter was separated anteriorly from the inferior vena cava. The delated ureter opened by vertical incision and the ureter was anteriorised and a ureteroureterostomy was done using 4-0 Vicryl. Tube drain was placed and wound was closed in layers. Drain was removed on the fiveth postoperative day. Patient was discharged on eighth postoperative day after suture removal. Discussion Retrocaval ureter is a rare congenital abnormality. Though the abnormality is congenital, it does not present until the third or fourth decades of life. The inferior vena cava normally develops from the posterior cardinal, subcardinal and supracardinal veins, which undergo sequential development, anastomosis and regression to become the inferior vena cava and azygous venous system. Normally the right subcardinal veins forms the pre renal inferior vena cava, the subcardinal -supracardinal anastomosis forms the renal segment and the right supracardinal vein forms the post renal inferior vena cava. Left supracardinal and lumbar portion of right posterior cardinal vein atrophy. If the subcardinal vein in the lumbar portion fails to atrophy and becomes primary right side vein, the ureter is trapped dorsal to it.1 Variations of this include duplication of vena cava with the ureter lying beside or behind the vascular limbs. There is a report of a case of left Retrocaval Ureter associated to a transpsition(Brooks),(8). Common presentations are right lumbar pain, dull aching or intermittent (renal colic), recurrent urinary tract infections and microscopic or gross haematuria. There is a high incidence of calculi due to stasis. Diagnosis is confirmed by ultrasonography and intravenous urography. Spiral CT scan and MRI help sometimes to delineate the anatomy clearly and non-invasively. Retrocaval ureter is classified into two types based on its radiographic appearance and the site of narrowing of ureter.4,5 Type I
Type II
The various anomalies associated with retrocaval ureter are Horse shoe kidney, Double IVC6 and Left retrocaval ureter with Goldenhar syndrome.7 Harril in 1940 emphasised that the position of the ureter and involved structures makes transection of the pelvis and re-anastomosis the most effective surgical treatment. Treatment entails dissecting the ureter anteriorly from the inferior vena cava, anteriorization and ureteroureterostomy. If there is severe hydronephrosis, Anderson Hynes pyeloplasty with pre caval transposition of the ureter has been advocated. Occasionally nephrectomy may be required in presence of thinned out cortex, poor function or severe infection. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09021f1.jpg] |
| |||||||||

{kind=link}