 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
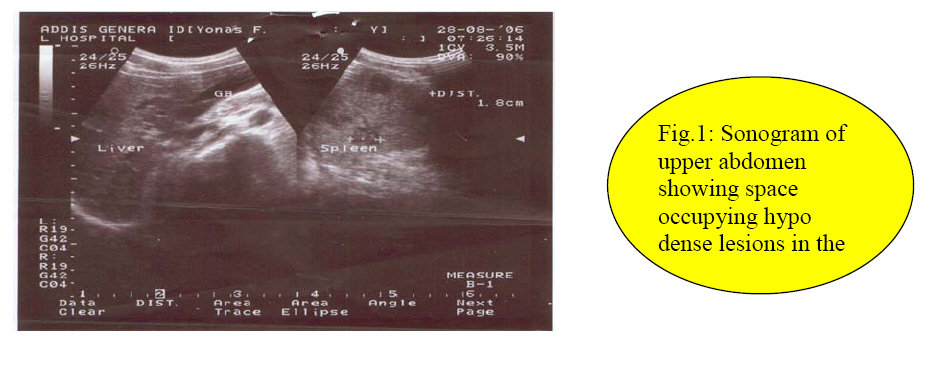
East and Central African Journal of Surgery, Vol. 14, No. 1, March-April 2009, pp. 122-123 HIV Related Isolated Tuberculosis of the Spleen: A Case Report S. Workneh1, A. Deneke2, B. Kotisso3 1Senior Surgical Resident, 2Consultant Surgeon, 3Consultant Surgeon, Head dep't of Surgery, St. Paul's Hospital; Addis Ababa University-Medical Faculty Code Number: js09022 A patient with left upper quadrant pain, intermittent fever, and weight loss but no radiographic evidence suggestive of pulmonary tuberculosis is presented. Abdominal sonography showed multiple hypo echoic nodular splenic lesions reported as foci of infection/abscess. Histopathology study of splenectomy specimen revealed caseous tuberculous lesions of near normal size organ. Introduction TB of the spleen is a rare disease except when involved in the process of miliary pattern 1. TB may be difficult to diagnose when it presents in an uncommon extra pulmonary site. Under such circumstances it may be right to suspect underlying immunosuppression and investigate for HIV infection which is the case with our patient. Case report A twenty-eight year old male patient presented with one month history of left lower quadrant abdominal pain, intermittent fever, anorexia, and weight loss. He strongly denied any history of cough, chest pain and bowel habit change. On examination, he was febrile, temperature 39.10C, and tachycardic but normotensive. No pallor, jaundice or lymphadenopathy. Chest exam was normal. Patient had no abdominal tenderness or palpable spleen. Except the vital signs and subjective complaints the man appeared clinically healthy looking. His hemoglobin was 12gm/dl, TLC 6,600/mm3, DLC: N= 68%, L= 32%, E=0% & M=0%. Chest radiograph PA and urinalysis did not show any abnormality. Abdominal sonography revealed minimally enlarged spleen with multiple small intraparenchyml hypo echoic lesions which were reported to be foci of infection otherwise abscess, biggest one measuring 1.8 cm in diameter. No ascites or other abdominal pathology detected. FNAC was not done. Splenectomy was done and specimen subjected for histopathologic examination. No intra abdominal lymphadenopathy or other pathology detected. Spleen weighed 160gms. Section showed foci of caseous necrosis rimed by epitheloid cells and Langhans giant cells. A diagnosis of caseous tuberculosis was made following which patient was put on antituberculous chemotherapy. Despite initiation of medical therapy patient continued to have fever which led to suspicion of other underlying infection and blood tested for HIV infection. The serum was reactive for HIV antigens. He then was started on HAART in another center. Note also that patient underwent laparotomy for perforated appendicitis after six months of splenectomy and had smooth course. Discussion Spleen can be involved in TB in one of the following three ways: miliary pattern, generalized caseating lymphadenitis or acute non-reactive hematogenous tuberculosis1. However, it is widely agreed that foci of hypo dense lesions in the substance of spleen is non specific and the list of differentials is many. So, ultrasound can not be the main stay of diagnosis in such cases. Some researchers strongly recommend FNAC of these lesions before definitive treatment1. But in one report from India the limitation of FNAC is noted by a non conclusive result1. Hence histopathology remains to be the final means to provide appropriate etiologic diagnosis. The absence of lymphadenopathy, pulmonary or other intraabdominal focus in our patient strongly suggests the diagnosis of primary TB involving the spleen as acute hematogenous tuberculosis. The fact that the patient turned out to be HIV positive indicates its relation with unusual primary TB. Therefore, we recommend that patients with unusual primary TB should be screened for HIV. References
© 2009 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js09022f1.jpg] |
| |||||||||

{kind=link}